A Previously Healthy Child with Allergic Aspergillosis
Abstract
Background:
Aspergillus
is a ubiquitous mold found in soil, decaying vegetation and indoor
environments. Its spores (conidia) are airborne and frequently inhaled. In
healthy individuals, these spores are cleared by innate immune defenses, but in
susceptible hosts, they can germinate and cause disease.
Keywords:
Pulmonary, Allergic, Alveoli, Sore throat, Aspergillosis
Abbreviations: ABPA:
Allergic Bronchopulmonary Aspergillosis; CF: Cystic Fibrosis; CT: Computed
Tomography CPA: Chronic Pulmonary Aspergillosis; IPA: Invasive Pulmonary
Aspergillosis
1. Introduction
1.1.
Background: Aspergillus is a ubiquitous mold found in
soil, decaying vegetation and indoor environments. Its spores (conidia) are
airborne and frequently inhaled. In healthy individuals, these spores are
cleared by innate immune defenses, but in susceptible hosts, they can germinate
and cause disease.
2. Case Presentation
We present a case study related to allergic aspergillosis, detailing the clinical history and examination results of a patient. The patient in question is a 13 years old male previously healthy, suffering from a cough for 10 days, general weakness and significant weight loss (5 kg). The medical treatment included cefotaxime but showed no improvement. Clinical examination revealed a high temperature (38°C - 38.5°C), headache, sore throat, paroxysmal cough and an overall decline in condition (Figure 1).

Figure 1: X RAYS at admission.
Chest CT scans displayed interest in the interstitium and alveoli, indicating dense central areas surrounded by low-density zones. There was notable pulmonary parenchymal density increase, suggesting inflammatory involvement and bilateral enlarged lymph nodes. Various other examinations were conducted, including blood tests that showed CRP 2.24 mg/dl, elevated total IgE levels (1117 IU/ml), IgG for aspergillus was positive, eosinophilia 17%, galactomannan antigen was positive (Figure 2).
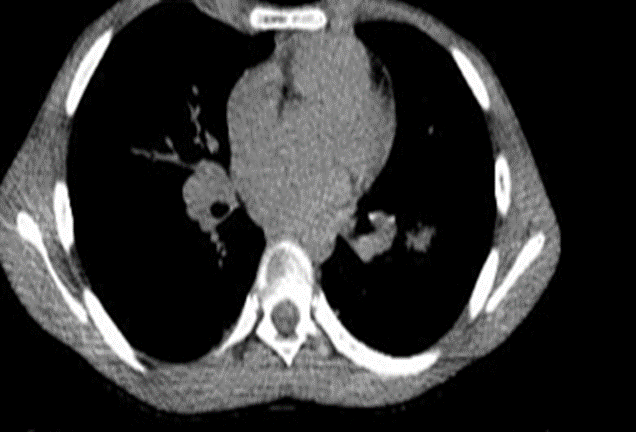
Figure 2: Computed Tomography scan.
Diagnosis
of allergic aspergillosis was made based on imaging, laboratory galactomannan
antigen, elevated IgE and positive specific aspergillus Ig G1-3. Treatment of ABPA consist on Corticosteroids
± antifungals (itraconazole, voriconazole) 4.
Treatment
efforts included oxygen therapy, prednisone being introduced at 35 mg per day
and itraconazole. The patient's condition fluctuated, exacerbating when the
prednisone dosage was decreased.
Follow-up
examinations corroborated the improvement of the patient's condition and
additional scans showed normal results, reflecting a positive response to the
adjusted therapy. Retrospective reports by family members revealed that the
patient had exposure to damp corn, which might have contributed to the allergic
reaction.
Overall,
the case illustrates the challenges and complexities involved in diagnosing and
managing allergic alveolitis, particularly in pediatric patients.
Pulmonary aspergillosis is a spectrum of lung diseases caused by infection or hypersensitivity to Aspergillus species, most commonly Aspergillus fumigatus. It can manifest in several clinical forms depending on the host’s immune status and underlying lung condition. Understanding its background requires looking at the pathogen, risk factors, disease types and pathophysiology4.
3. Discussion
Allergic Bronchopulmonary Aspergillosis (ABPA) is a pulmonary disease caused by Aspergillus induced hypersensitivity that occurs in immunocompetent but susceptible patients with asthma and/or Cystic Fibrosis (CF)1. Pulmonary aspergillosis is classified into distinct entities:
- Allergic Bronchopulmonary
Aspergillosis (ABPA): Hypersensitivity reaction to Aspergillus antigens in Asthma2, cystic fibrosis clinically by wheezing, bronchiectasis,
recurrent pulmonary infiltrates. Allergic disease: Immune dysregulation with
Th2-mediated hypersensitivity, elevated IgE and eosinophilia3.
- Chronic Pulmonary
Aspergillosis (CPA): Localized infection in pre-existing lung cavities in patients
with prior TB, COPD, sarcoidosis clinically with cavitary lesions, hemoptysis,
weight loss, fatigue.
- Aspergilloma, fungal ball colonizing a pre-existing cavity. Structural lung disease often asymptomatic, but hemoptysis can occur.
- Invasive Pulmonary Aspergillosis (IPA): Angioinvasive infection with tissue necrosis. Severely immunocompromised (neutropenic, transplant). Fever, cough, pleuritic chest pain, hemoptysis, rapidly progressive respiratory failure.
Treatment of different forms of aspergillosis in children:
ABPA Corticosteroids
± antifungals (itraconazole, voriconazole).
CPA/Aspergilloma: Long-term
antifungal therapy; surgical resection in selected cases.
IPA: Voriconazole is first-line; amphotericin B or isavuconazole as alternatives4.
Adjunctive:
Reduction
of immunosuppression, surgical intervention for massive hemoptysis.
Pulmonary aspergillosis represents a continuum of disease ranging from hypersensitivity to life-threatening invasive infection. The clinical outcome depends heavily on host immunity, early recognition and appropriate antifungal therapy.
4. References
- Agarwal R,
Chakrabarti A. Allergic
bronchopulmonary aspergillosis in children: An update. Pediatric Allergy and Immunology.
2022.
- Manti S, Parisi GF, Papale M, et
al. Salvatore Leonardi. Allergic bronchopulmonary
aspergillosis in children.
- Stevens DA. Cystic
fibrosis and ABPA: Diagnostic and therapeutic advances. Clinical Microbiology Reviews, 2021.
- Shah
A, Panjabi C. ABPA in children:
Clinical perspectives. World
Allergy Organization Journal. 2020.