Orthopaedic Complications in Infancy
Abstract
Orthopaedic complications encountered during infancy include a broad spectrum of positional deformities, congenital anomalies, developmental disorders and neuromuscular conditions affecting the musculoskeletal system. Positional deformities such as intoeing, metatarsus adductus, talipes equinovarus, calcaneovalgus, genu varum, genu valgum and pes planovalgus are commonly observed during early childhood and are often associated with intrauterine positioning or physiological developmental variations. While many of these conditions resolve spontaneously with growth, persistent or progressive deformities may require conservative management orthotic intervention, physiotherapy, serial casting or surgical correction. Developmental dysplasia of the hip remains one of the most important orthopaedic disorders of infancy because early diagnosis and treatment are critical for normal hip development and prevention of long-term disability. In addition, neuromuscular and congenital conditions, such as arthrogryposis multiplex congenita, may result in severe joint contractures, muscle weakness and functional limitations that require multidisciplinary rehabilitation. This review summarises the aetiology, clinical presentation, assessment methods, imaging modalities, treatment approaches and rehabilitation principles of common orthopaedic complications observed in infancy. Emphasis is placed on early recognition, physiotherapy management orthopaedic indications and long-term functional outcomes.
Keywords: Infancy, Orthopaedic
complications, Intoeing, Femoral anteversion, Tibial torsion, Metatarsus
adductus, Talipes equinovarus, Developmental dysplasia of the hip, Pes
planovalgus, Arthrogryposis multiplex congenita, Physiotherapy, Pediatric orthopaedics
Abbreviations: AMC:
Arthrogryposis Multiplex Congenita; CNS: Central Nervous System; CT: Computed
Tomography; DDH:
Developmental Dysplasia of the Hip; HKAFO:
Hip Knee Ankle Foot Orthosis; KAFO: Knee Ankle Foot Orthosis;
LLD: Leg Length Discrepancy; MRI: Magnetic Resonance Imaging; MTA: Metatarsus
Varus or Metatarsus Adductus; PPV: Pes Planovalgus; TEV: Talipes Equinovarus;
US: Ultrasonographic; LLD: Leg Length Discrepancy
1. Introduction
Orthopedic
problems observed during infancy are classified into two groups. The first
group comprises positional problems arising from a restricted intrauterine
environment. The second group comprises defects involving true congenital
anomalies.
1.1. Intoeing
Torsional deformities of
the long bones of the lower extremities may lead to gait abnormalities and
joint pain in children. Increased femoral anteversion and excessive internal
tibial rotation frequently coexist and are defined as malalignment of the lower
extremity1,2.
In the clinical condition
referred to as intoeing, three conditions may be present: femoral anteversion, internal
tibial rotation and metatarsus adductus. In many children, this condition
resolves spontaneously by the age of 8
years old without treatment and is now considered part of normal
development1. However, in
children with persistent intoeing, serial casting may be applied for metatarsus
adductus, whereas rotational osteotomies may be performed for internal tibial
torsion and femoral anteversion.
1.2. Femoral Anteversion
The femoral anteversion
angle is defined as the angle formed between the two most posterior points of
the femoral condyles and the midpoint axis of the femoral neck and shaft.
Newborns typically have 25° to 35° of
femoral anteversion and 0° of tibial torsion.
During the first 5 years of life, femoral version decreases to approximately 16°, while the tibia undergoes external rotation up to
20°1,3.
Intoeing observed during infancy, decreased external tibial rotation is most commonly present. However, intoeing observed during childhood is generally associated with increased femoral anteversion and increased soft-tissue tightness (Figure 1).

Figure 1: Increased femoral anteversion4.
In the presence of femoral anteversion, the hip undergoes compensatory in Internal rotation during gait to preserve the lever arm of the hip abductors. During walking, insufficient knee extension mechanics become apparent during the transition from mid-stance to terminal stance. In addition, internal tibial torsion is frequently observed. Children with femoral anteversion commonly prefer the W-sitting position for comfort5. However, there is currently no scientific evidence regarding the consequences of this sitting posture (Figure 2).

Figure 2:
W-sitting with increased femoral anteversion5.
To evaluate the femoral anteversion angle, the amount of hip internal rotation is measured3. For this assessment, the child is placed in the prone position with the knees flexed to 90°. The greater trochanter is palpated to detect movement and the hip is passively internally rotated. Internal rotation exceeding 45° indicates increased femoral anteversion (Figure 3). During the evaluation, the thigh-foot angle and foot progression angle are also important and should normally range between 5° and 30° (Figure 4). By approximately age 8, the angle is expected to decrease to less than 10°C. In the presence of symptoms such as pain or asymmetry, consultation with an orthopedic specialist is strongly recommended. Surgical indications include severe and persistent tibial or femoral torsion after the age of 8 years, a thigh–foot angle of less than 15° and hip internal rotation greater than 80° after the age of 10 years. Torsional deformities of the femur and tibia can be evaluated using low-dose computed tomography. The functional effects of these deformities can be demonstrated through three-dimensional gait analysis by assessing joint range of motion, joint moments and power generation.

Figure 3: Measurement of femoral anteversion4.

Figure 4: Foot progression angle: The angle between the long axis of the thigh and the long axis of the foot (the axis running from the centre of the heel to the space between the second and third toes)6.
1.3. Tibial Torsion
Alignment of the lower leg is
determined by identifying the hip–foot axis, which is used to define the
orientation of the tibia. Tibial torsion is defined as the angle between the
two most posterior proximal points of the tibia and the most prominent lateral
point of the ankle joint (lateral malleolus)7.
In essence, lower extremity alignment is determined by the degree of rotation
between the proximal and distal ends of the tibia, which represents a
structural characteristic of the tibial bone itself (Figure
5). Tibial torsion is commonly evaluated by measuring the angle between
the thigh's longitudinal axis and the malleolar axis with a goniometer, while
the child is prone with the knees flexed7
(Figure 6). Some researchers alternatively
define tibial torsion as the angle between the axis passing through the knee
and the axis connecting the medial and lateral malleoli when both the hip and
knee are flexed to 90° (Figure
7). In infants, the tibia is generally internally rotated due to
intrauterine positioning. During growth, the long axis naturally derotates.
External tibial torsion develops during the first 6 months following the onset
of independent walking and continues until approximately 18 months of age1,7. At birth, the thigh-foot angle is
approximately −15° (normal range: −30° to +20°), whereas at
3 years of age it is approximately +5° (normal
range: −10° to +20°).
During childhood, normal alignment is characterized by external tibial torsion
ranging from 0° to +30°, most commonly around 10°.
In recent years, studies have also assessed tibial torsion using Computed Tomography (CT), Magnetic Resonance Imaging (MRI) and three-dimensional gait analysis. Goniometric measurements of tibial torsion in children have been reported to range between 0° and 45°.

Figure 5: Internal tibial torsion (where the foot’s angle of progression is within normal limits but there is external rotation at the knee)4.
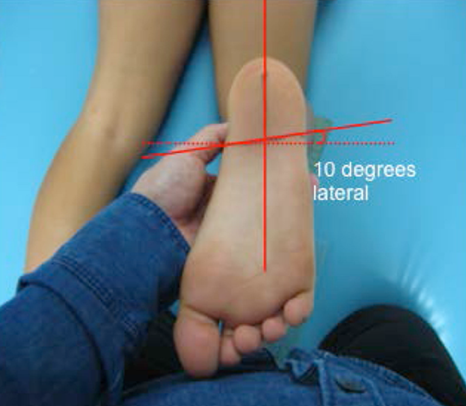
Figure 6: Indirect measurement of tibial torsion using the angle between the malleoli and the long axis of the femur7.

Figure 7: Indirect measurement of tibial torsion using the angle between the malleoli and the long axis of the femur7.
Infants with internal tibial torsion have shortened extremity rotator muscles in the hip. The infant’s lower extremities are positioned in abduction and external rotation. In physiotherapy, treatment options are limited to stretching the hip and lower extremity muscles toward internal rotation and implementing weight-bearing exercises after 6 to 7 months of age; complete correction is generally not achieved. Until approximately 6 months of age, a Denis Browne splint, which maintains the lower extremities in external rotation during sleep, may be used. In later stages, these children may be treated surgically with external rotation osteotomy of the tibia and fibula. In adulthood, increased internal tibial rotation has been associated with knee osteoarthritis and patellar instability. Out-toeing is most commonly caused by excessive external tibial torsion, decreased femoral version or shortening of the hip musculature.
1.4. Metatarsus Adductus
Metatarsus Varus or Metatarsus Adductus (MTA) is one of the most common positional problems in infants, with an incidence of approximately 1-2 per 1,000 live births. It has also been reported to result from a developmental abnormality of the medial cuneiform bone. The deformity is characterized by adduction or medial deviation of the forefoot starting from the tarsometatarsal joint. Associated soft tissue tightness leads to secondary osseous adaptations. Full ankle dorsiflexion range of motion is typically preserved1. During clinical assessment, the heel bisection line can be used. With the knee flexed to 90°, a line is drawn from the midpoint of the heel on the plantar surface toward the forefoot and the medial deviation of the forefoot relative to this line is evaluated. Normally, this line passes through the second toe. The condition is classified into three grades: mild, moderate and severe (Figure 8). In mild cases, the line aligns with the third toe; in moderate cases, with the fourth toe; and in severe cases, with the fifth toe. Some clinicians also use Grade 1/2 to describe dynamic MTA, in which the foot appears normal at rest but dynamic forefoot varus and medial deviation of the hallux are observed during gait. Mild cases do not require treatment and typically resolve spontaneously by 4-6 months of age8. Moderate cases may respond to stretching exercises and to corrective footwear, such as straight- or reverse-last shoes. Severe cases can be managed with manipulation, serial casting and corrective footwear. However, both mild and moderate forms of MTA generally resolve spontaneously by 3-4 years of age without intervention. Cases that fail to resolve spontaneously may later require surgical correction9.

Figure 8: Degrees of metatarsus adduktus10.
1.4.1. Talipes Equinovarus: Talipes Equinovarus (TEV), also known as clubfoot and often confused with Metatarsus Adductus (MTA), was first described by Hippocrates as medial deviation of the forefoot, a small calcaneus, hindfoot varus and ankle equinus. The foot and calf on the affected side are typically smaller compared to the contralateral side. In some children, TEV may be associated with conditions such as myelomeningocele, developmental dysplasia of the hip and arthrogryposis. The deformity is classically characterized by hindfoot equinus and varus, midfoot cavus and forefoot adduction11,12. Typical congenital TEV is thought to result from a combination of genetic predisposition and environmental factors such as abnormal intrauterine constraint, maternal smoking during pregnancy, maternal age, alcohol consumption and oligohydramnios. Approximately 80% of cases are idiopathic and a positive family history is present in about 25% of cases. The incidence is approximately 1 per 1,000 live births, with a male-to-female ratio of 2:1. The most commonly used clinical scoring systems include the Pirani score and the Dimeglio classification, which assess severity based on the physical characteristics of the foot13. The primary treatment approach is the conservative Ponseti technique. The Ponseti method consists of two phases:
Correction
phase: This includes manipulation, serial
casting, bracing and percutaneous Achilles tenotomy. It typically lasts about
the first 3 months of life.
Maintenance phase: The foot is maintained in a corrected position using a foot abduction orthosis. The orthosis is initially worn for 23 hours per day during the first 12 weeks and subsequently used as a nighttime splint until 4 to 5 years of age. Functional exercises are initiated once the child begins weight-bearing.
The method is highly
effective and surgical intervention is rarely required. Manipulations mainly
consist of traction applied in the opposite direction to the deforming forces acting
on the foot and typically last about 30 minutes. These include talonavicular
joint correction, derotation of the calcaneo-forefoot complex, stretching of
the Achilles tendon, lengthening while preserving the midtarsal joint,
stretching of the medial arch and plantar fascia and passive mobilization into
plantarflexion and dorsiflexion12,14.
In addition to the Ponseti method, other approaches such as the Robert Debré
method, the Saint Vincent de Paul method and the Montpellier method have been
described.
If 90° of ankle
dorsiflexion cannot be achieved after rehabilitation, a percutaneous Achilles
tenotomy is performed. In some cases, additional procedures such as subtalar or
tibiotalar capsulotomy or a mini-incision release of the plantar fascia may be
required to improve joint flexibility further. Once the child achieves
independent and appropriate gait mechanics, physiotherapy sessions are
discontinued and the patient is transitioned to a home exercise program with
follow-up visits at monthly or 3-month intervals. Night splinting is continued
until approximately 4-5 years of age.
1.4.2. Calcaneovalgus:
It is a commonly observed positional problem in newborns. In this condition, the
forefoot is laterally deviated, the hindfoot is in valgus and excessive ankle
dorsiflexion is present. At birth, the dorsum of the foot is in contact with
the anterior aspect of the lower leg. Positional calcaneovalgus typically
resolves spontaneously without intervention. It should be distinguished from
calcaneovalgus secondary to vertical talus. In vertical talus, the talus is
positioned vertically and the navicular is displaced dorsally. While the
forefoot is dorsiflexed, the hindfoot is in plantarflexion. This condition,
referred to as a “rocker-bottom foot” deformity, is typically rigid.
1.4.3. Genu varum:
To assess genu varum, the infant is placed in the supine position and the
medial malleoli are brought together. One hand is used to stabilize the ankles
by keeping the malleoli in contact. The distance between the medial femoral
condyles is then measured. The infant’s lower extremities should be fully
exposed and no diaper should be present during the assessment. In crying or
restless infants, a triangular measuring device may be more practical, enabling
quicker, more efficient measurements.
Physiological
genu varum does not require treatment if it persists beyond 2 years of age or
worsens progressively and it typically resolves spontaneously15 (Figure 9). These
infants are generally developmentally normal for motor milestones. In some
cases, treatment may involve a Hip Knee Ankle Foot Orthosis (HKAFO) or a Knee-Ankle-Foot
Orthosis (KAFO). Surgical intervention is rarely required. If genu varum
persists and progresses beyond 4 years of age, the child should be evaluated
for systemic disorders, such as vitamin D resistant rickets. Blount disease
(also known as idiopathic tibia vara) is another condition characterized by
genu varum, resulting from growth suppression of the proximal tibial epiphysis15. Medial metaphyseal fragmentation may
also be observed in this condition. In infants younger than 3 years with Blount
disease, a rigid HKAFO worn for 23 hours per day is recommended. In some cases,
a proximal tibial osteotomy may be required. Genu varum may also be observed in
the presence of chondromalacia.

Figure 9: Genu varum10.
Indications for orthopedic evaluation in genu varum are as follows:
Positive family history of pathological genu varum
Asymmetric deformity, including unilateral involvement, gait
abnormalities or leg length discrepancy
Persistent varus deformity at approximately 8 months of age
without resolution
Short stature below the 25th percentile
Inability to walk after 18 months of age
Localized Blount’s varus angle in the proximal tibia
Progressive varus deformity persisting beyond 18 months of
age
Persistence of varus alignment beyond 24 months of age
1.4.4. Genu valgum: Like
genu varum, genu valgum is not expected to persist beyond 2 years of age. After
this age, progressive genu valgum may be observed in overweight children,
children with an out-toeing foot progression angle and in cases following
fractures or trauma, osteomyelitis and in children with pes planovalgus. The
condition is assessed with the infant in either the supine or standing position.
During measurement, the medial femoral condyles are brought into contact and
the intermalleolar distance is measured. In cases of severe genu valgum or genu
varum, guided growth techniques may be applied during adolescence by
temporarily tethering the growth plate16.
This allows continued growth on the untethered side of the femoral physis,
resulting in gradual correction and restoration of proper lower limb alignment.
1.4.5. Pes planovalgus: Pes Planovalgus (PPV) is
defined as the collapse of the medial longitudinal arch, hindfoot valgus and
forefoot abduction and supination. For physiotherapists, PPV is important for
achieving proper biomechanical alignment of the lower extremities in infants.
In children with flexible pes planovalgus, the medial longitudinal arch appears
normal when sitting or standing on tiptoes; however, it collapses when weight
is fully applied to the foot17.
These children are often hypermobile and may demonstrate features of
generalized ligamentous laxity, such as the ability to flex the wrist and touch
the forearm with the thumb, as well as hyperextension at the knees and elbows.
Physiological flatfoot is common in infants and affects approximately 45% of
preschool-aged children. In contrast, pathological pes planus is rigid and
requires intervention. The medial longitudinal arch typically develops rapidly
between 2 and 6 years of age. In painless flexible pes planus, no treatment is
required and arch development occurs spontaneously17,18.
In such cases, there is no indication for footwear modifications, insoles or
orthoses. It has been shown that the use of corrective shoes or insoles before age
3 does not affect arch development and these children demonstrate outcomes
similar to those of untreated controls. A higher prevalence of pes planovalgus
has been reported in children who begin wearing shoes before the age of 6 and
in obese children after the age of 6. Shoes supporting the medial longitudinal
arch may be recommended; however, they do not facilitate arch formation but may
reduce pain by improving biomechanical alignment. In symptomatic flexible
flatfoot, conservative management may include rest, activity modification,
massage and exercise therapy17.
Although insoles, shoes or orthoses do not directly promote arch development,
they may help reduce pain by improving biomechanical function. In adulthood, a
high arch has been reported to cause greater pain and functional impairment
than a low arch. Unless associated with other orthopedic or neurological
conditions, pes planovalgus is now considered part of normal development in
early childhood and no intervention other than lightweight running shoes is
generally required. After the age of five, shoes with medial arch support may
be recommended to promote proper biomechanical alignment of the lower
extremities19.
Achilles tendon
contracture or shortening may lead to secondary pes planovalgus. Examples of
conditions associated with this include cerebral palsy, congenital tight heel
and muscular dystrophies. Fixed hindfoot valgus may result in pain, callus
formation, ulceration and poor tolerance to orthotic devices. These conditions
can be corrected with Achilles tendon lengthening procedures and other soft-tissue
or bony interventions when necessary.
In cases
of Pes Planovalgus (PPV), increased femoral anteversion and external tibial
torsion may also be observed concurrently (Figure 10).

Figure 10: In association with Pes Planovalgus (PPV), increased femoral anteversion and external tibial torsion may also be present19.
1.4.6. Developmental dysplasia of the hip: Developmental Dysplasia of the Hip (DDH) is synonymous with congenital hip dysplasia and is defined as abnormal development of the femoral head and acetabulum, usually accompanied by joint laxity20,21. It has been reported to occur at a rate of 4 per 1,000 live births22. In DDH, the acetabular index angle is increased and may progress to subluxation and dislocation over time20,21. The acetabular index angle demonstrates the inclination of the acetabulum in the frontal plane. It is the angle between Hilgenreiner’s line and a line parallel to the acetabular roof passing through the superolateral edge of the acetabulum20 (Figure 11).

Figure 11: Acetabular index angle24.
Normal hip development requires normal muscle balance and a femoral head deeply seated within the acetabulum20,21. The formation of a concave acetabulum develops through a spherical femoral head. Identification of hip dysplasia during the neonatal period and initiation of treatment are important for normal hip joint development20,23. During the early fetal period (6 to 20 weeks), the amount of femoral head coverage and acetabular anteversion does not vary and the hip appears well covered. A fetal dislocated hip becomes apparent only during the last trimester20. Predisposing factors for DDH in infants may be classified as mechanical, physiological and environmental factors20,24. Mechanical factors include limited intrauterine space and a tight abdominal wall during the first pregnancy, oligohydramnios, breech presentation and positioning of the fetal hip within the mother’s sacrum. Physiological factors include maternal hormones such as estrogen and relaxin, which cause ligamentous laxity in female infants. Due to this factor, the female-to-male ratio in DDH is considered to be 6:1. Environmental factors include tightly wrapping the infant’s lower extremities in extension by methods such as swaddling after birth20,24. Problems associated with DDH include congenital muscular torticollis, metatarsus adductus and calcaneovalgus21,24.
1.4.7. Assessment: The newborn hip may be classified as follows20,24:
Normal - non-instability
Subluxatable: The femoral head is
within the socket but can partially move out of the acetabulum.
Dislocatable: The femoral head is
reduced but becomes dislocated with the Barlow maneuver.
Dislocated but reducible: The
femoral head is outside the acetabulum at rest but can be reduced with the
Ortolani maneuver.
Dislocated and irreducible: This is rarely encountered after the second month of life. This type of dislocation is mostly teratologic, occurs before birth and is associated with a neurological or muscular anomaly such as myelomeningocele or arthrogryposis20,21.
During the clinical assessment, hip
abduction in flexion is evaluated. Most infants have 75°
to 90° of abduction. An asymmetry or limitation
of 5° to10° may
indicate hip dysplasia25. Other
clinical findings include asymmetric thigh folds, apparent femoral shortening
characterized by inequality of knee levels (Galeazzi sign) and positive Barlow
and Ortolani signs20,24.
The Galeazzi sign is considered positive
when one knee remains higher than the other after both hips and knees are flexed
to 90°, indicating leg length discrepancy. The
dislocated hip remains more posteriorly positioned and the leg appears shorter20,24.
For the Barlow and Ortolani tests, the infant
should be completely relaxed23,24
(Figure 12). Even the slightest contraction
around the hip may mask instability. The findings of these two tests assessing
hip instability disappear around 2 to 3 months of age because either hip
stability increases and the femoral head settles into the acetabulum or the hip
becomes fixed in the dislocated position20,24.
In the Barlow test, direct posterior pressure is applied to the femoral head
from the acetabulum to determine whether it can be displaced out of the
acetabulum23,24. In infants older
than one month, limitation of hip abduction is usually the only finding. During
evaluation of hip abduction, the infant lies supine and the pelvis is
stabilized while the hips are in 90° flexion.
One hip is then abducted. If hip abduction is less than 45°-60° or if there is a
20° difference between the abduction of the two
hips, the hip must be examined thoroughly24,25.
However, it should be remembered that DDH is bilateral in approximately 20% of
cases20.

Figure 12: Ortolani Test (A) and Barlow Test (B). In the Ortolani maneuver, the hip flexed to 90° is abducted while anteriorly directed pressure is applied proximally. In the Barlow maneuver, the hips flexed to 90° are adducted while moderate posteriorly directed pressure is applied24.
Ultrasonographic
(US)
evaluation of the infant hip is currently very common and is a routine practice26-28. US is faster and more useful than
other radiographic methods and is used until the age of 3 to 6 months, before
the femoral head ossifies and obscures the visualisation of deeper structures.
US enables visualisation of cartilaginous structures that cannot be seen on
plain radiographs without radiation exposure and stress tests can also be
performed simultaneously26,27. In
addition to aiding diagnosis, it also demonstrates the extent of progress
achieved during treatment27.
Bilateral dislocations should also be considered in infants. If abduction of
both hips is less than 60°, radiographic
examination should be performed24,25.
An acetabular index angle below 30° is
considered normal, between 30° to 40° suspicious and
above 40° pathological. In older children,
especially after 1 year of age, anteroposterior hip radiography is preferred.
In this radiograph, the acetabular index angle is considered valuable. It has been
stated that the acetabular index angle decreases with age and is used as an
assessment parameter for determining hip development20,21. According to radiographic findings,
the hip is classified as mild radiological deviation, minor joint instability,
acetabular dysplasia (without subluxation or dislocation), subluxated or
dislocated20. Cardiac anomalies, Talipes
Equinovarus (TEV) or renal anomalies may accompany the condition22. If left untreated, it may lead to damage
of the hip joint cartilage and functional loss of movement20,24.
2. Treatment
2.1. From
birth to 6 months of age
The Pavlik harness is a frequently
used method for hip reduction in DDH29,30.
In recent years, treatment protocols have involved monitoring the hip during
the first 4 to 6 weeks after birth before initiating Pavlik harness treatment31. In 70% to 90% of cases, hip instability resolves spontaneously
within 2 to 4 weeks25,31. Infants
whose hips remain unstable after 4 to 6 weeks of age are treated with a Pavlik
harness. The Pavlik harness prevents hip extension and adduction, thereby
maintaining the hip in flexion and abduction. The flexion and abduction
position supports normal acetabular development and helps facilitate kicking
movements. Due to the biological plasticity of the developing bone, positioning
the hip in flexion/abduction supports acetabular development24,30. The reason for preferring the Pavlik
harness is that it allows active hip movement and reduces the risk of avascular
necrosis30,31. Complications
associated with the use of the Pavlik harness include avascular necrosis of the
femoral head, femoral nerve palsy, pressure ulcers, musculotendinous
shortening, inferior dislocation and erosion of the posterior rim of the
acetabulum24,29. The Pavlik
harness is generally used between the 6th and 12th
weeks after birth with ultrasonographic follow-up of the hip. If
no improvement in hip development is observed following its use, surgical
treatment is indicated29. Other
orthoses that may be alternatives to the Pavlik harness include the Craig
orthosis and the Von Rosen splint24.
2.2. After
6 months of age
In infants between 6 and 18 months of age diagnosed with a dislocatable or dislocated hip, surgical intervention is generally required. In infants with hip instability after 6 months of age, closed reduction/stabilization under anesthesia is performed. If the procedure is successful, a spica cast (abduction cast) maintaining the hip at 90° to 100° flexion is applied for 6 weeks32 (Figure 13).

Figure 13: Spina Cast.
During walking, pelvic obliquity, leg length discrepancy and increased lumbar lordosis are the most prominent findings. A Trendelenburg gait is observed due to weak hip abductors and hip flexion contracture20,24. If closed reduction is unsuccessful, open reduction surgery is performed. Open reduction is especially preferred in children older than 18 months32. In most cases, a pelvic osteotomy called Salter osteotomy is performed32,33 (Figure 14). In this technique, an osteotomy is performed on the pelvic bone above the acetabulum. Subsequently, the distal segment is displaced laterally, anteriorly and inferiorly32. Following open reduction, a spica cast is also used for 6 weeks, after which physiotherapy is initiated33. In particular, if a dysplastic hip with subluxation is left untreated, articular cartilage damage develops in late adolescence. Degenerative arthritis and hip and extremity pain may develop20,33. Very mild dysplasia, however, may remain asymptomatic for years and individuals may experience only hip joint degeneration20.

Figure 14: Salter osteotomy33.
2.2.1. Idiopathic toe walking: Some infants may walk on their toes during the early stages of gait development. This condition may occur even in the absence of a history of prematurity, difficult delivery or hypertonia34,35. Interventions that can be applied for infants with “idiopathic toe walking” include:
Plantar surface, foot and calf
massage,
Normal ankle joint range-of-motion
exercises,
Weight-bearing activities, cruising
and gait training on different surfaces while barefoot to promote lower
extremity loading (such as sand, sponge, quilt or mat surfaces),
Use of first-step shoes or
orthopedic boots.
Most infants respond positively to these interventions35,36.
3.
Arthrogryposis Multiplex Congenita (AMC)
Arthrogryposis Multiplex Congenita
(AMC) is a non-progressive neuromuscular syndrome37,38.
The term originates from the Greek words “arthron” and “gryposis,” which mean
“curved” or “hooked” joints. AMC is characterized by congenitally shortened
muscles, non-progressive limitation of joint movements and thickening of the
periarticular capsules involving two or more joints37. This condition
results in severe joint contractures, muscle weakness and fibrosis20,21,37,38. Subluxation or dislocation may
occur in the hip, knee and patella20,37.
Long-term outcomes may lead to severe disability and limitations in mobility
and activities of daily living38,39.
The incidence is approximately 1 in every 3,000-4,000 live births, with equal
prevalence in male and female infants. In 50% to 60% of cases, all four
extremities are affected, whereas 30% to 40% involve only the lower extremities
and 10% to 15% involve only the upper extremities40.
The etiology remains unknown;
however, multiple factors during the first trimester of pregnancy are thought
to contribute to the condition. Decreased fetal movement is considered a
primary cause of multiple joint contractures. Some mothers of infants with AMC
report febrile illnesses lasting 1-2 days during pregnancy. Prenatal viral
infections, vascular abnormalities between the mother and fetus and uterine
septum anomalies are among the suspected etiological factors. Diagnosis may
involve muscle biopsy, blood tests and genetic analyses37.
AMC can be classified into
amyoplasia (classic arthrogryposis), distal arthrogryposis, neuromuscular
syndromes and Central Nervous System (CNS)
arthrogryposis. Amyoplasia is the most common subtype, accounting for approximately
three-quarters of all cases37. In
amyoplasia, clubfoot deformity, elbow extension contracture, shoulder internal
rotation and adduction, forearm pronation and hip flexion-external rotation
contractures are commonly observed37,40.
The involvement is generally symmetrical. Distal arthrogryposis primarily
affects the hands and feet and demonstrates autosomal dominant inheritance.
Neuromuscular AMC is associated with neurogenic and myopathic disorders. Muscle
weakness reduces fetal joint movement, leading to joint stiffness and
deformities. Muscle imbalance in the extremities causes postural deviations
toward the weaker muscles. During the last trimester, decreased amniotic fluid
and fetal growth further restrict fetal movements. CNS arthrogryposis results
from developmental abnormalities affecting the frontal lobe, such as
hydranencephaly and microcephaly37.
3.1. Clinical findings
Severe joint contractures and
deficient muscle development or amyoplasia are commonly observed. Two clinical
patterns are most frequently encountered. In the first pattern, the child
presents in a flexed posture with hip dislocation, knee extension, equinovarus
deformity, shoulder internal rotation, elbow flexion and wrists positioned in
flexion with ulnar deviation. In the second pattern, the hips are abducted and
externally rotated, the knees flexed and the shoulders internally rotated and
adducted, while the elbows remain extended and the wrists flexed with ulnar
deviation. Additional findings may include scoliosis, skin dimpling over
joints, hemangioma, decreased finger creases, congenital heart defects, facial
anomalies, respiratory problems and abdominal hernias37,40. It should also be noted that these
patients are at risk for scoliosis progression and temporomandibular joint
involvement37,38.
3.2. Medical treatment
The primary component of medical
management is appropriately timed surgical intervention. Surgical procedures
may include correction of equinovarus deformity, Achilles tendon lengthening,
surgical treatment of hip dislocation, surgical treatment of knee flexion
contractures and tendon transfers to obtain elbow flexion. When conservative
splinting and stretching fail, wrist fusion in a functional position may be
performed40.
3.3. Physiotherapy and rehabilitation
The primary responsibility of the rehabilitation
team is to educate the family about AMC39,40.
Families should be informed that the disease is non-progressive; however,
without proper positioning, stretching and strengthening exercises, functional
limitations cannot be prevented. Physiotherapy assessment may include
goniometric measurements of the joints and motor development evaluations40. Motor development is frequently delayed
in these infants38,39. Infants with
AMC commonly present with equinovarus deformity, hip flexion contracture, knee
extension contracture, shortening of the internal rotators of the shoulder and
elbow and wrist flexion contractures37,40.
Most of these infants are born in breech presentation37.



Figure 15: Deformities observed in AMC38.
The aims of physiotherapy are to
increase muscle strength and joint range of motion, support overall
sensorimotor development and educate families regarding positioning and
stretching techniques. Interventions may include positioning the infant in age-appropriate
functional postures, stretching exercises, splinting, gross and fine motor
exercises and sensory integration therapy39,40.
Prone positioning during the first
three months is particularly important for preventing hip flexion contractures.
These infants often achieve mobility on the floor by moving while sitting on
their hips. Surgery for equinovarus deformity should ideally be performed
before 2 years of age to allow soft-tissue procedures rather than bony surgery40. Most children achieve independent
ambulation by approximately two years of age38,40.
Families should be encouraged to support standing activities beginning at six
months of age40. For infants who
are unable to stand after 18 months, a standing frame may be appropriate39,40.
Fine motor exercises are important
for functional activities such as feeding and should therefore begin as early
as possible39,40. Stretching exercises
should be performed in 3 to 5 sets, with each stretch maintained for 20 to 30
seconds40. In children with AMC,
stretching exercises are lifelong interventions and regular stretching during
the first two years is particularly important39,40.
Splints should be used to maintain continuity of stretching. The stretching
force of splints should not be adjusted to the end range of motion immediately;
instead, the stretching intensity should be gradually increased every 4 to 6
weeks40.
Foot and ankle orthoses should be
used for approximately 22 hours per day. Particularly during the first 3 to 4
months after birth, anterior knee flexion splints or posterior knee extension splints
should be worn for approximately 20 hours daily. In older infants, knee flexion
splints exceeding 50° should be avoided to prevent hip flexion contractures.
Knee extension splints may be used after the fourth month during standing
activities and sleep. Hand and wrist splints are generally appropriate after
the third month, allowing the infant time to develop normal physiological
flexion patterns. For daytime use, a neutral-position splint providing gentle
extension stretch, placed dorsally and supporting the palmar arches, may be
preferred, while a stretching hand-wrist splint may be used at night.
Functional hand-wrist splints, maintaining the hand and wrist in an optimal
functional position, may also be beneficial during daytime activities40.
4. Other
Orthopedic Problems
4.1. Osteomyelitis
Osteomyelitis is an infection of the
bone caused by bacterial organisms. It may spread from the metaphyseal bone to
adjacent joints. It can progress rapidly and destructively, leading to
permanent complications. It most commonly occurs in the distal femur and
proximal tibia. The onset of infection is usually hematogenous and may occur
secondary to microorganisms entering the body through the skin, infected wounds
or the throat. Symptoms include high fever, pain, tenderness and swelling in
the affected metaphyseal region41,42.
4.2. Septic arthritis
Septic arthritis is an infection of
a joint caused by bacteria. It may cause joint degeneration within 48 hours of
symptom onset. Permanent gait problems may develop due to cartilage damage. The
hip joint is the most commonly affected joint, followed by the knee. In
neonates, septic arthritis of the hip is particularly destructive because of
complete damage to the cartilaginous femoral head. Even mild cases may lead to
permanent complications, as increased intra-articular pressure can result in
avascular necrosis. Fever and avoidance of using the affected extremity are
commonly observed43.
4.3. Transient synovitis
Transient synovitis is one of the
most common causes of hip pain in children. It is more frequently seen in boys.
It may occur secondary to another infection elsewhere in the body and is
characterized by joint pain. The condition usually resolves spontaneously
within one week44.
4.4. Occult fracture
Hairline fractures, particularly
those referred to in English as “toddler’s fractures,” are examples of occult
fractures. The infant may refuse to walk and there may be no obvious history of
trauma, fever or signs of infection. Occult fractures are often recognized
retrospectively when callus formation begins in the bone. Treatment includes
splinting or casting45.
4.5. Kohler syndrome
Kohler syndrome is an
osteochondroses affecting the navicular bone. Pain is present over and around
the navicular bone. On radiographic examination, the navicular bone appears
sclerotic and reduced in size. The disease generally resolves spontaneously
over time46.
4.6. Achondroplasia
Achondroplasia (dwarfism) is an
autosomal dominant disorder within the broad group of osteochondrodysplasias.
Characteristics of this disorder include cuboid-shaped vertebral bodies,
causing narrowing of the spinal canal, lumbar lordosis, short tubular bones and
short hands. Neurological damage associated with spinal anomalies may be
observed in 20% to 47% of cases. There are marked differences in the
proportions of the extremities and trunk. Hypotonia and transient kyphosis are
present in most of these infants47,48.
4.7. Leg length discrepancy
Leg Length Discrepancy (LLD) is defined as a difference greater than 2.5 cm between the two lower extremities. It may result from traumatic, congenital, neuromuscular, acquired diseases or infections49. Treatment may be conservative or surgical. Surgical management includes shortening the longer extremity or lengthening the shorter extremity. Before surgery, physiotherapy interventions include muscle strengthening, passive range-of-motion exercises, sensory training, stabilization exercises and weight-bearing activities on the shorter extremity. In the postoperative period, positioning, splinting, stretching and strengthening exercises are applied. Functional activities, active-assisted and isometric exercises, gait training, bicycle ergometer and treadmill applications are commonly used rehabilitation approaches50,51.
5. References
- Gonzales AS,
Mendez MD. Intoeing (Pigeon Toes, Femoral Anteversion, Tibial Torsion,
Metatarsus Adductus). StatPearls Publishing. 2019.
- Hudson D. The rotational
profile: A study of lower limb axial torsion, hip rotation and the foot
progression angle in healthy adults. Gait Posture. 2016;49: 426-430.
- Hefti
F. Pediatric Orthopaedics in Practice. 2nd ed. Springer. 2015.
- Harris
E. The intoeing child: etiology, prognosis and current treatment options. Clinics in podiatric medicine and surgery. 2013;30(4): 531-565.
- Sielatycki
JA. W-sitting in childhood: a systematic review.
- Shin CS,
Chaudhari AM, Andriacchi TP. Valgus plus internal rotation moments increase
anterior cruciate ligament strain more than either alone. Medicine and science in sports and exercise. 2011;43(8): 1484-1491.
- Borish
CN, Mueske NM, Wren TAL. A comparison of three methods of measuring tibial
torsion in children. Clin Anat. 2017;30(8): 1043-1048.
- Allen WD, Weiner DS,
Riley PM. The treatment of rigid metatarsus adductovarus with the use of a new
hinged adjustable shoe orthosis. Foot Ankle. 1993;14(8): 450-454.
- Herzenberg JE, Burghardt
RD. Treatment of resistant metatarsus adductus: casting versus orthosis. J Orthop
Sci. 2014;8(2): 193-201.
- Rerucha CM, Dickison C,
Baird DC. Lower Extremity Abnormalities in Children. Am Fam Physician. 2017;96(4):
226-233.
- Diméglio A, Bensahel H,
Souchet P, et al. Classification of clubfoot. J Pediatr Orthop B. 1995;4: 129-136.
- Cooper DM, Dietz FR.
Treatment of idiopathic clubfoot: a thirty-year follow-up note. J Bone Joint
Surg Am. 1995;77: 1477-1489.
- Diméglio A, Bonnet F,
Mazeau P, et al. Orthopaedic treatment and passive motion machine: consequences
for the surgical treatment of clubfoot. J Pediatr Orthop B. 1996;5: 173-180.
- Garcia-Gonzalez NC,
Hodgson-Ravina J, Aguirre-Jaime A. Functional physiotherapy method results for
the treatment of idiopathic clubfoot. World J Orthop. 2019;10(6): 235-246.
- Dettling S, Weiner DS.
Management of bow legs in children: A primary care protocol. J Fam Pract.
2007;66(5): E1-E6.
- Ballal MS, Bruce CE,
Nayagam S. Correcting genu varum and genu valgum in children by guided growth.
J Bone Joint Surg Br. 2010;92(2):273-276.
- Carr JB, Yang S, Lather
LA. Pediatric pes planus: a state-of-the-art review. Pediatrics. 2016;137(3): 2015-1230.
- Akcali O, Tiner M,
Ozaksoy D. Effects of lower extremity rotation on prognosis of flexible
flatfoot in children. Foot Ankle Int. 2000;21: 772-774.
- Cebulski-Delebarre A,
Boutry N, Szymanski C, et al. Correlation between primary flat foot and lower
extremity rotational misalignment in adults. Diagn Interv Imaging. 2016;97(11):
1151-1157.
- Dezateux C, Rosendahl K.
Developmental dysplasia of the hip. Lancet. 2007;369(9572):1541-1552.
- Aronsson DD, Goldberg MJ,
Kling TF Jr, et al. Developmental dysplasia of the hip. Pediatrics. 1994;94(2):
201-208.
- Bialik V, Bialik GM,
Blazer S, et al. Developmental dysplasia of the hip: a new approach to incidence.
Pediatrics. 1999;103(1): 93-99.
- American
Academy of Pediatrics Committee on Quality Improvement, Subcommittee on
Developmental Dysplasia of the Hip. Clinical practice guideline: early
detection of developmental dysplasia of the hip. Pediatrics. 2000;105(4): 896-905.
- Jackson JC, Runge MM, Nye NS. Common questions about
developmental dysplasia of the hip. Am Fam Physician. 2014;90(12): 843-850.
- Shipman SA, Helfand M, Moyer VA, et al. Screening for
developmental dysplasia of the hip: a systematic literature review for the US
Preventive Services Task Force. Pediatrics. 2006;117(3): 557-576.
- Graf R. The diagnosis of congenital hip-joint dislocation by
the ultrasonic Combound treatment. Arch Orthop Trauma Surg. 1980;97: 117-133.
- Clarke NMP. Sonographic clarification of the
problems of developmental dysplasia of the hip. J Bone Joint Surg Br.
2001;83(3): 423-430.
- Shorter D, Hong T, Osborn DA. Screening programmes for
developmental dysplasia of the hip in newborn infants. Cochrane Database Syst
Rev. 2011;(9): CD004595.
- Mulpuri K, Song KM, Goldberg MJ, et al. Detection and
nonoperative management of pediatric developmental dysplasia of the hip in
infants up to six months of age. J Am Acad Orthop Surg. 2015;23(3): 202-205.
- Cashman JP, Round J, Taylor G, et al. The natural history of
developmental dysplasia of the hip after early supervised treatment in the
Pavlik harness. J Bone Joint Surg Br. 2002;84(3): 418-425.
- Cook KA, Schmitt M, Ingram M, et al.
Pavlik Harness initiation on Barlow positive hips: Can we wait? J Orthop.
2019;16(5): 378-381.
- Vitale MG, Skaggs DL.
Developmental dysplasia of the hip from six months to four years of age. J Am Acad Orthop Surg. 2001;9(6): 401-411.
- Esmaeilnejad-Ganji
SM, Esmaeilnejad-Ganji SMR, Zamani M, et al. Modified Salter Osteotomy
Technique for Developmental Dysplasia of Hip. Biomed Res Int. 2019;2019: 6021271.
- Freiman
HD, Mensah C, Codrington J, et al. Idiopathic Toe-Walking in Children and
Adolescents: Diagnosis, Natural History and Treatment Options. JBJS Rev.
2022;10(2).
- Williams C, Tinley P, Rawicki B. Idiopathic toe walking - are
common podiatric treatment options based on evidence? J Foot Ankle Res.
2013;6(1): 037.
- van
Kuijk AA, Kosters R, Vugts M, et al. Treatment for idiopathic toe walking: a
systematic review of the literature. J Rehabil Med. 2014;46(10): 945-957.
- Hall JG.
Arthrogryposis (multiple congenital contractures): diagnostic approach to
etiology and classification. Eur J Med Genet. 2014;57: 464-472.
- Dahan-Oliel
N, Bedard T, Darsaklis VB, et al. Development of a research platform for
children with arthrogryposis multiplex congenita. BMJ Open. 2018;8(6): 021377.
- Elfassy
C, Darsaklis VB, Snider L, et al. Rehabilitation needs of youth with
arthrogryposis multiplex congenita. Disabil Rehabil. 2019.
- Donohoe M, Bleakney DA. Arthrogryposis Multiplex Congenita.
In: Campbell SK, editor. Physical Therapy for Children. WB Saunders. 2000.
- Dartnell
J, Ramachandran M, Katchburian M. Haematogenous acute and subacute paediatric
osteomyelitis: a systematic review of the literature. J Bone Joint Surg Br.
2012;94(5): 584-595.
- Peltola
H, Paakkonen M. Acute osteomyelitis in children. N Engl J Med. 2014;370: 352-360.
- Sultan J, Hughes PJ. Septic arthritis and acute osteomyelitis
in children. BMJ. 2010;340: 66.
- Fischer
SU, Beattie TF. The limping child: epidemiology, assessment and outcome. J Bone
Joint Surg Br. 1999;81(6): 1029-1034.
- Dunbar
JS, Owen HF, Nogrady MB, et al. Obscure tibial fracture of infants: the
toddler’s fracture. J Can Assoc Radiol. 1964;15: 136-144.
- Mubarak SJ, Carroll NC. Kohler’s disease and Freiberg’s
disease. Orthop Clin North Am. 1976;7(4): 983-1002.
- Pauli
RM. Achondroplasia: a comprehensive clinical review. Orphanet J Rare Dis. 2019;14:
1.
- Ireland PJ, Donaghey S, McGill J, et al. Development in
children with achondroplasia: a prospective clinical cohort study. Dev Med
Child Neurol. 2012;54(6): 532-537.
- Gurney
B. Leg length discrepancy. Gait Posture. 2002;15(2): 195-206.
- Paley D.
Current techniques of limb lengthening. J Pediatr Orthop. 1988;8(1): 73-92.
- Sabharwal S, Kumar A. Methods for assessing leg length discrepancy. Clin Orthop Relat Res. 2008;466(12): 2910-2922.