Complications During Pregnancy Among Indian Tribal Women: A Mini-Review
Abstract
This study highlights the
complications during pregnancy among disadvantaged tribal mothers of India. Findings
are based on recently published research articles from 2020 to 2025. The tribal mothers are majorly
affected by Anaemia (29.5% to 94.6%), Hypertension (11.69% to 28.57%), Preterm
labour (50.73%), Vaginal Bleeding (33.3%), intrauterine growth restriction (IUGR)
(29.5%) and Abdominal pain (33.3%) complications during pregnancy followed by other
problems like GDM (Gestational Diabetes Mellitus) (14.2%), Excessive Vaginal
Discharge (8.33%), etc. Community-based
intervention and improved outreach health services can help reduce the burden
of pregnancy-related complications, prevention and management in rural tribal settings.
Keywords: Complications during pregnancy, Tribal mothers, MCH services, India
1. Introduction
The maternity life of a woman begins with pregnancy,
and that time requires access to regular antenatal check-ups for foetus growth
and the well-being of women. With the support of adequate nutrition (one extra
meal) and regular antenatal check-ups to ensure the healthy development of both
the child and mother. This will prevent life-threatening complications.
However, tribal women, who often reside in remote and inaccessible regions,
face significant challenges in accessing these essential services. The lack of
healthcare infrastructure, nutritious diet, basic medication, and routine
check-ups contributes to a high prevalence of pregnancy-related complications
among tribal women, rendering them more vulnerable than their non-tribal
counterparts. Owing to poor connectivity and underdeveloped health systems,
particularly in rural and remote areas, tribal populations are more suffer to
avail modern health facilities. The status of tribal women is vulnerable,
characterized by low literacy rates, involvement in agricultural labour, and
poor socio-economic conditions in India. Their utilisation of maternal and
child health (MCH) services is disproportionately low, largely due to their
geographical isolation and limited resources. Though tribal communities display
diverse livelihoods, socio-economic conditions remain largely uniform, with
only slight variations. According to the Ministry of Tribal Affairs, Government
of India, tribal populations constitute 8.6% of India's total population, with
a literacy rate of 73.60% (80.40% male, 66.70% female). Furthermore, the
Agricultural Census 2015–2016 reveals that 56.26% of the tribal population is
engaged in marginal agricultural activities, while only 0.75% are involved in
large-scale agriculture.1 Health indicators also reflect the
disadvantaged health status of indigenous (tribal) populations. The key
indicators, such as the Total Fertility Rate (TFR), Infant Mortality Rate
(IMR), and Under-Five Mortality Rate, are higher along with poor nutritional status
when compared with the mainstream population1.
While all women may experience health issues during
pregnancy, tribal women are disproportionately affected by diseases,
nutritional disorders, and limited access to treatment. The reasons behind primarily
due to poor road conditions and a lack of public transportation facilities to
reach health centres. Mishra PS et al. reported that low utilization of
maternal healthcare services in hilly regions, with only 19% of tribal women
accessing antenatal care services during pregnancy2.
Hence, the likelihood of experiencing pregnancy-related complications,
such as hypertensive disorders, anaemia, and intrauterine growth restriction
(IUGR), is notably higher among tribal mothers3.
India officially recognizes over 700 tribes, many of
which inhabit remote and difficult terrains and remain largely disconnected
from the mainstream population. While the country has achieved milestones such
as reaching the moon, significant gaps remain in effectively connecting and
empowering to tribal population. To address
these concerns, the Government of India (GOI) has implemented various
initiatives, such as the National Health Mission, Poshan Abhiyan, and Janani
Suraksha Yojana, aimed at combating malnutrition, anaemia, and financial
barriers to healthcare. Nevertheless, out of the 10.45 crore tribal population,
5.20 crore are women who remain underrepresented in policy discussions and
interventions4. The study of
Adolescent Girls of Indigenous Communities in Telangana (2024) examined the
prevalence, causes, and determinants of chronic malnutrition, assessed through
stunting, thinness, and underweight among adolescent indigenous girls.
Additionally, the sociocultural focus on starchy, staple-based diets and early
marriage influenced the outcomes5.
Furthermore, Tribal women also face an elevated risk of depression and
anxiety during maternity; however, these conditions are often neglected in
public health interventions. Maternal mental health disorders during pregnancy,
in particular, impair key caregiving behaviours that are critical for child
survival6. The paper by Kumar, D. et
al. (2025) also highlighted the growing risk of hypertension among the tribal
population, which is a serious concern that demands urgent attention7.
A secondary review using Penchansky and Thomas’s
framework identified that the major barriers to healthcare utilization among
tribal women lie in the dimensions of Accessibility, Availability, and
Acceptability. These factors were found to have a more profound impact on
healthcare access than Accommodation and Affordability8. This article consolidates findings
from existing peer-reviewed literature to highlight the recent major
pregnancy-related complications and barriers faced by tribal women in India,
aiming to inform more inclusive health policy and targeted interventions.
2. Methodology
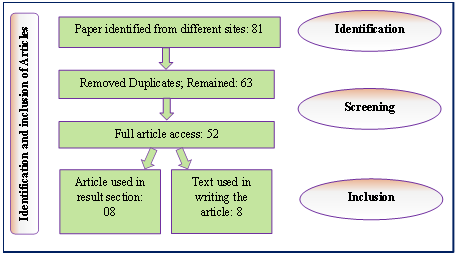
In the process of collecting data from secondary sources, we followed a structured procedure for identifying published articles across various search engines, including PubMed, Google Scholar, Research Gate, Science Direct, JSTOR, Semantic Scholar, CORE, and Google Search. We used specific keywords such as "pregnancy-related complications," "perinatal risks/complications," "complications during the antenatal period," "tribal women," "scheduled tribes," "tribal people," "tribal population," "Indigenous people," in India focusing on publications from 2020 to 2025. Priority was given to original research articles. Following our criteria, we initially identified 81 articles. These were then screened, and duplicates were removed, resulting in 63 articles. After further review, we gained full access to 52 of these articles. In the final step, we selected 08 articles for inclusion in the data table, while the remaining articles were referenced in the write-up. The process is summarized in the organogram presented as (Figure 1).
|
|
3. Result
Prenatal (during pregnancy) complication and
utilization of MCH services assessed through published research articles since
last 5 years from different regions of India shown in table-1. Finding revealed
that the tribal women during the pregnancy were more sufferer with Anaemia ranging
from 29.5% to 94.6%, Hypertension (11.69% to 28.57%), Preterm labour (50.73%),
Vaginal Bleeding (33.3%), IUGR (29.5%), Abdominal pain (33.3%). Followed by
others problems GDM (Gestational Diabetes mellitus) (14.2%), Excessive Vaginal
Discharge (8.33%), HBV Infection (7.1%), Spontaneous Abortions (3.30%), Heart
Disease (2.38%), Birth asphyxia (1.54%) and Advanced resuscitation (1.40%). Use
of MCH services during the pregnancy were found 23% of tribal mothers received
antenatal care services and 82% were hospital birth, and only 52% children of
age one year received birth dose vaccination. It was reported that 39% faced
challenges in accessing the MCH services, 46% related to transportation and 23%
unavailability of hospital-based services during the COVID-19 pandemic period.
Hence, tribal people have the option to avail primary treatment from Traditional healers as
a point of care in tribal areas to cure a range of health issues, including
non-communicable diseases like type II diabetes.
Table 1: Distribution of complications/illness during pregnancy and utilisation of MCH services.
|
Sl. No. |
Population |
Study Site |
Study Year |
Prenatal
Complication |
|
1 |
Tribal population |
Gujrat |
2021 |
Anaemia (45.90%),
Hypertension at delivery (11.69%), Birth asphyxia (1.54%), advanced
resuscitation (1.40%)9 |
|
2 |
Tribal population |
Kerala |
2020 |
Hypertension
(28.57%), Gestational Diabetes Mellitus (GDM) (14.2%), Anaemia (29.5%), intrauterine growth restriction (IUGR) (29.5%), Preterm Labour (50.73%),
HBV infection (7.1%), and heart disease (2.38%)3 |
|
3 |
Tribal population |
Maharashtra |
2021 |
Vaginal Bleeding
(33.3%), Abdominal Pain (33.3%), Excessive Vaginal Discharge (8.33%),
Spontaneous Abortions (3.30%)10 |
|
4 |
Tribal population |
Rajasthan |
2023 |
Anaemia (94.6%)11 |
|
5 |
Tribal population |
India |
2021 |
Traditional
healer(s), provide primary healthcare. The traditional healers provide a cure
for a range of health issues, including non-communicable diseases like type
II diabetes12 |
|
6 |
Tribal population |
Andhra Pradesh,
Assam, Jammu and Kashmir, Karnataka, Madhya Pradesh, Maharashtra, Odisha,
Rajasthan, and Uttarakhand. |
2023 |
52% of children were
fully vaccinated by the age of 12 months among the tribal populations; 11%
did not receive any vaccine, and 37% of the tribal children received some
vaccines13 |
|
7 |
Tribal population |
Maharashtra, Odisha,
Assam, Uttar Pradesh, Madhya Pradesh and Telangana |
2023 |
|
|
8 |
Tribal population |
India |
2024 |
Only 23% of the
mothers received adequate antenatal care. 82% were institutional childbirths15 |
4. Discussion
These mini-reviews of research findings have confirmed
that tribal women are more suffer from Anaemia (29.5% to 94.6%) and Hypertension
(11.69% to 28.57%), which may be responsible for considerably higher preterm
labour (50.73%). Maternal illiteracy, clinical anaemia, and lack of antenatal
care (ANC) are all significant independent risk factors for preterm delivery9. Pregnancies with complications and high risks
must be managed through essential emergency obstetric services, including
specialized nursing care to decrease perinatal risks16. These risk factors are likely influenced by systemic and structural
discrimination, which continues to generate disparities in access to maternal
health services. Additionally, complications during pregnancy may arise from
spontaneous or induced abortions, especially when carried out by untrained
personnel in unsafe environments or through unsafe methods, which are frequent
in remote or tribal settings. These complications can include bleeding,
infection, pain regardless of the provider or setting, and the lack of post abortion
care (PAC), including emergency care, counselling, and linkage to health
services, further increases risks10.
Access to maternal and child health (MCH) services in tribal and
marginalized communities is hindered by a complex interplay of socio-cultural
norms, infrastructural limitations, and educational gaps. The key barriers are
outlined below:
4.1. Socio-cultural and traditional influences
A significant proportion of girls (19.5%) in tribal
areas marry at an early age between 10 to 17 years, leading to early and
high-risk pregnancies11. This
contributes to adverse maternal and neonatal outcomes and reduces the
likelihood of adequate antenatal care. Also forced to mobilise towards dependence on Traditional Healers, they
serve as the first point of contact for many tribal populations, offering
spiritual and cultural health support. However, their lack of formal
integration into the public health system can result in delays in seeking
appropriate medical care12.
4.2. Lack of awareness and health literacy
Many families are unaware of maternal health schemes,
financial incentives, and services provided by the government, which leads to
underutilization of available resources. In addition, with low levels of education among women and
limited knowledge among male family members about pregnancy-related
complications, decrease in timely health-seeking behaviour. Poor road
conditions and limited or delayed ambulance services hinder timely access to
healthcare facilities, especially during pregnancy-related emergencies. In addition, digital health services offer
potential healthcare, but they are often inaccessible in tribal areas due to
poor network connectivity, low technological literacy, and a lack of
infrastructure to support telemedicine platforms. In this regard, the COVID-19
pandemic highlighted the need for stronger infrastructure, adequate staffing,
and resilient service delivery to ensure the continuity of MCH services during
health emergencies14. Improving
maternal and child health (MCH) services requires a culturally sensitive and
community-based approach. One key strategy is the integration of traditional
healers into the formal health system. By engaging them as Tribal Health
Ambassadors through incentive-based models, early referrals and knowledge
sharing can be improved. Post-Abortion Care (PAC) must be strengthened to
include emergency treatment, infection management, contraception counselling,
and effective referrals, especially in rural and tribal regions where unsafe
abortions are common.
5. Conclusion
During the pregnancy, tribal mothers are considerably
affected by Anaemia, Hypertension, Preterm birth, etc. Awareness and education
campaigns are essential to increase health knowledge among tribal women.
Enhancing transport infrastructure and ensuring reliable ambulance services are
vital for timely access to institutional care. Promoting female education and
male involvement in reproductive health can lead to better health-seeking behaviour
in favour of the reduction of morbidities and complications during pregnancy.
6. Acknowledgement
The authors acknowledge the Indian Council of Medical
Research (ICMR)-National Institute of Research in Tribal Health (NIRTH),
Jabalpur, for encouragement and technical support.
7. Conflict of Interest
The authors have no conflict of interest.
8. References
- Ministry of
Tribal Affairs - Government of India. Statistics. Accessed, 2025.
- Mishra
PS, Pautunthang N, Marbaniang SP. Geographical divide led inequality in
accessing maternal healthcare services between hills and valley regions of
Manipur state, India. Clin Epidemiol Glob Health, 2021;11: 100744.
- Jayasree S, Suneela MS. Maternal
complications among tribal women in a tertiary care centre. Int J Clin Obstet
Gynaecol, 2020;4: 342-346.
- Sahal
K. Status and main issues of tribal women in India.
- Ravula P,
Kasala K, Pramanik S, et al. Stunting and Underweight among Adolescent Girls of
Indigenous Communities in Telangana, India: A Cross-Sectional Study. Nutrients,
2024;16: 731.
- Singh
T, Kumar D. Children under 5-year mortality and the risk of maternal mental
illness among India’s scheduled tribe. Indian J Psychiatry, 2025;67: 350-353.
- Kumar D,
Singh T. The growing risk of hypertension in India’s Scheduled tribes. Hypertense
Res, 2025;48: 345-352.
- Abedin
Z, Asif, Hemant. On the margins: exploring barriers to health service
accessibility for tribal women in India. Hum Geogr, 2024;18: 1-20.
- Shah S,
Desai S, Desai T, et al. Trends and risk factors in tribal vs nontribal preterm
deliveries in Gujarat, India. AJOG Glob Rep, 2021;1: 100026.
- Chhabra
S, Suman A. Community-based study of abortion complications and care sought by
rural tribal women of an extremely low resource setting. Gynecol Obstet Reprod
Med. Published online, 2021: 1-7.
- Dwivedi R,
Goel AD, Vyas V, et al. Gap identification for improvement in maternal and
early infant health care practices among tribal pregnant women in an
aspirational tribal district Sirohi, Rajasthan. J Family Med Prim Care,
2023;12: 3291-3297.
- Saxena
N, Kumar D, Das A. Connecting the unconnected: the way forward for public
health to reach the unreached tribal communities in India. Curr Sci, 2021;120.
- Kusuma YS,
Kumari A, Rajbangshi P, et al. Vaccination and associated factors
among tribal children of 1 year age in nine Indian districts: a cross-sectional
study. Trop Med Int Health, 2023;28: 530-540.
- Sharma S,
Aggarwal S, Kulkarni R, et al. Challenges in accessing and delivering maternal
and child health services during the COVID-19 pandemic: a cross-sectional rapid
survey from six states of India. Int J Environ Res Public Health, 2023;20.
- Kusuma YS, Kumari A, Rajbangshi P, et al. Maternal healthcare seeking and determinants of adequate antenatal care and institutional childbirth among Indian tribes: a cross-sectional study from nine districts. Eur J Obstet Gynecol Reprod Biol, 2024;292: 163-174.
- Singh T, Kumar D. Perinatal risk in India’s Scheduled Tribes. Lancet, 2024;404: 933-934.