Prevalence, Risk Factors and Interventions: Systematic Review of Maternal Mental Healthcare Access
Abstract
Maternal mental health is a critical yet often overlooked component of perinatal care, shaped by a dynamic interplay of cultural traditions, healthcare access and biological risk factors. This project explores how culturally embedded postpartum practices, such as Nigeria’s Omugwo, China’s zuo yuezi and South Asia’s Jaapa, can both protect against and contribute to postpartum depression (PPD). While these traditions foster familial support and emotional recovery, they may also discourage medical engagement or amplify stigma around psychiatric illness. In contrast, biomedical models in high-income countries emphasize standardized screening and pharmacologic or psychotherapeutic interventions, but often overlook the protective role of community and cultural continuity. PPD, now encompassed within the broader term perinatal depression, affects women globally, with higher rates in under-resourced settings. Disparities in the prevalence of PPD emphasize the urgency of culturally responsive screening and treatment. Risk factors include prior mental illness, birth trauma such as emergency C-sections, sleep disruption and insufficient social support. Despite validated tools like the Edinburgh Postnatal Depression Scale and emerging therapies including oral Zuranolone, PPD remains underdiagnosed, particularly amongst immigrant and minority populations. This project therefore proposes a novel, integrative framework for maternal mental health that values both cultural tradition and biomedical innovation. By reframing maternal recovery through both clinical and cultural lenses, we can reduce stigma, improve diagnosis and optimize postpartum outcomes across global contexts.
Keywords: Maternal mental health, Postpartum mental health, Mental Healthcare Access, Systemic Barriers, & Perinatal Behavioral Health
1.
Background
Maternal
health outcomes vary significantly across different cultural, geographical and
socioeconomic contexts, influenced primarily by socio-cultural practices,
quality of healthcare systems and traditional beliefs
and values. The study of Perinatal Mood and Anxiety
disorders or PMADs, have been a growing area of study
in recent years
and refers to the overall
umbrella of depression and anxiety concerns during pregnancy1. The World Health Organization determined
that approximately 1 out of 10 pregnant women and 1 out of 13 postpartum women
have reported experiencing depressive symptoms,
with higher rates in developing countries. The onset
of perinatal and postpartum depression poses dangers both to infant and
maternal health, with severe cases often resulting in maternal suicide and poor
infant development2. Despite the scale
of this issue, approximately 50% of cases are untreated and undetected3. At a greater
risk of developing these issues are individuals of a lower socioeconomic
status, victims of violence, those lacking adequate social support and
immigrants4. Researchers have
also determined that complications during pregnancy or delivery, poor diet and
a history of depression are more susceptible to developing postpartum
depression4.
Immigrant populations specifically are subject to greater challenges in accessing maternal healthcare, which impact their pregnancy outcomes1. Interventions to maternal mental crises also vary between cultures, with some opting to utilize prayer, meditation and alternative therapies over drug-based or traditional therapeutic intervention1. Ultimately, cultural deviations in medical practices around maternal health can serve either as a protective or limiting factor in achieving optimal outcomes for both the mother and the infant.
Treatment of maternal mental health disorders are challenging to standardize across communities as well, given that providers have to tailor treatment plans to align with the individual’s unique condition and background. Despite therapy, counseling and antidepressants being established as relatively effective treatments, issues in accessibility for vulnerable populations still remain5.
2.
Discussion
2.1.
Perinatal depression & Other maternal mental health disorders
Postpartum
depression (PPD), now included in the term perinatal depression, is a
psychiatric disorder that affects 10-15% of new mothers worldwide6. It can affect individuals during pregnancy or within the first year after childbirth3. Although
PPD carries a high risk of
maternal mortality due to its strong correlations with suicidal ideation, it
remains understudied and underdiagnosed7,8.
Most new mothers experience the “postpartum blues” immediately following
childbirth which is composed of stress, sadness, anxiety, loneliness and
fatigue.
According to the Fifth Edition of the Diagnostic and Statistical Manual of Mental Disorders Text Revision (DSM-V-TR), the “postpartum blues” are not a mental disorder and do not cause functional impairment9. If these symptoms do not subside within two weeks, it can lead to PPD.
Multiple etiologies have been implicated in the development of PPD. This includes environmental factors, genetics, epigenetics, hormonal shifts and neuroendocrine mechanisms. However, there are no proven relationships between these factors and PPD8. Regarding environmental factors, in many countries like the United States, China, United Kingdom and India, PPD is highly stigmatized due to family, public and self-stigma10. This prevents many women from reaching out for help despite the availability of treatments11. In Georgia specifically, the percentage of postnatal women who reported feeling depressed or hopeless increased by 13% between 2017 and 202112. This is important to note as in 2010, Amnesty International listed Georgia and the District of Columbia as equally having the worst maternal mortality rates in the U.S13. Strong correlations are present between maternal mortality and PPD in the first year after diagnosis and over 40% of counties in Georgia are known as maternity care deserts, devoid of birthing hospitals or obstetric care. Thus, it is crucial to address potential barriers to care for maternal mental health in the state of Georgia to improve perinatal outcomes14,15.
Other environmental factors such as having a difficult childbirth, relationship problems, lack of support, social adversity or even self-blame can lead to PPD. The frequency of these specific psychosocial stressors strongly correlates to the country where the mother grew up due to the particular region’s cultures and traditions16. For example, in India there is immense value placed on women having sons. As a consequence, gender preference becomes a major contributor to PPD in Indian cultures17.
Although there are no definitive correlations between genetics and epigenetics in the risk of PPD, a 2013 study by Guintivano, et al. helped show that certain changes to chromatin structure are associated with PPD18. In this study with mice, it was found that individuals at risk for PPD may be more sensitive to estrogen-mediated epigenetic changes at the heterochromatin protein 1, binding protein 3 (HP1BP3) and tetratricopeptide repeat domain 9B (TTC9B) genes8. More studies need to be done to find causes for PPD.
A higher risk of suicidal ideation (SI) is associated with women experiencing PPD. In a study comparing the prevalence of SI in 5,688 Japanese postpartum women with and without depression, it was discovered that the SI of women with depression was 51.8% compared to only 3.3% in women without depression7. Not only does untreated PPD increase the risk of SI, but it can also lead to increases in child abuse and child neglect. Sometimes, women can develop postpartum psychosis after childbirth. Postpartum psychosis (PPP) is defined as a severe mental illness and psychiatric emergency indicated by symptoms of paranoia, hallucinations, obsessive thoughts about one’s child or attempts to harm oneself or the child19,20. Since PPP does not have a category in the DSM-V-TR, clinicians may fail to diagnose this condition. PPP occurs in 1 in 500 to 1 in 1000 deliveries and tends to be more common in primiparous women. The risk of recurrence of postpartum psychosis is 30-50% in women who experienced it in their first pregnancy9.
There is a 1-4.5% risk of infanticide in women with inadequately treated PPP21. Infanticide is often the result of the mother experiencing hallucinations and delusions that their child is evil or not their own22. On June 20, 2001 andrea Yates drowned her five children in a bathtub. She suffered from postpartum depression and was consequently found not guilty by reason of insanity23. When PPP goes undiagnosed, which it often does, it can intensify and lead to mothers harming themselves or their baby as shown in the case with Andrea Yates. It is essential that patients presenting symptoms of psychosis undergo a thorough history and neuropsychiatric evaluation so they are correctly diagnosed and treated20.
2.2.
Risk factors for maternal mental health
The
risk factors for women who will experience changes to their mental health are
dependent on several factors including community/social support, domestic
violence, financial security and many more24.
Several studies suggest that women who have stable community support (stable
relationship or familial support) are at a decreased risk for mental illness
postpartum24. Collectivist cultures are those
in which people
are a part of a strong community from birth and emphasis is
placed on family integrity and the success of the group over the individual25. In cultures with collectivist cultures,
family members aside from the parents commonly participate in childcare
responsibilities, providing social support to the mother, thus decreasing the
prevalence of PPD in these communities. For example, 10% of Ugandan women,
where collectivist culture is prominent, were
found to have a depressive illness while 13.1% of Portuguese women were found
to have PPD in urban Portugal, where collectivist culture is less prominent26. Additionally, Hispanic women
who immigrated to the US, were found to have a higher prevalence of PPD, 53%, as a result of a lack of
extended family support and potentially lower socioeconomic status26. This is an indication that a lack of
social support is a key risk factor for maternal mental health. In some
cultures where the idea of collectivism is prominent face a decrease in diagnosis as a result of
stigma surrounding mental health; however, the strong
social support is a preventative measure against mental health complications
after childbirth4.
Additionally, women who live in high income countries are at a significantly lower risk for mental health conditions postpartum27. Southern Africa has the highest prevalence of PPD (nearly 40%) and Spain has the lowest prevalence (9.09%)27. This is also indicative that income and regional development is relevant to mental health risk. Developed countries saw a lower prevalence of PPD (15%) while underdeveloped regions saw an increased prevalence (20%), with the average being 17% of women worldwide experiencing PPD27. This is a result of several factors, such as higher income being linked to increased access to quality healthcare and higher education level, both of which are also risk factors for maternal mental health. In the state of Georgia, an association for the comorbidity of hypertension and mental illness during pregnancy was found and the prevalence for this was found to be greater than twice as high in rural areas as opposed to large metro areas28. The health outcomes for mothers in Georgia is directly related to healthcare access and proximity29. Participants in a qualitative study determined that there were problems with the appropriateness of care because it varied across counties, especially in rural areas. In terms of mental health, there is a lack of mental health care centers in the state of Georgia, thus forcing people to travel far to receive care30. As shown on the maps in the Findings, the location of mental health care centers are far apart and there are very few in rural and socioeconomically vulnerable communities. Therefore, being in those areas decreases likelihood for diagnosis and treatment of mental health conditions. Physical health of the mother can also play a role in the risk for mental health disorders.
Trauma during birth, such as emergency cesarean sections versus normal birth conditions can also affect the mother’s risk for postpartum depression. C-sections are linked with post-traumatic stress disorder after birth, which often leads to PPD31. Women who underwent emergency C-sections had increased PTSD scores (by 0.47) on the PDSQ scale than women who underwent planned C-sections31. PTSD affects 4-17% of mothers postpartum and is a strong predictor of PPD31. Low quality of sleep due to increased disturbances throughout the night leading to decreased sleep duration was measured by the Pittsburgh Sleep Quality Index (PSQI) and determined that of the 75% of patients at risk for PPD 97.2% of patients reported disrupted sleep32. Furthermore, women who experience depressive symptoms are also less likely to get quality sleep, resulting in a cycle of poor sleep and depressive symptoms32. Previous history of mental health issues, specifically depression, is the highest indicator for PPD31.
2.3.
Cultural and societal perspectives on maternal mental health
Maternal mental
health is often a sector
of healthcare that goes unnoticed
across cultures; it
highlights a phase of life during extreme transition from prenatal to
postpartum, affecting mental and physical health alike. With up to 20% of women
suffering from mood or anxiety disorders during pregnancy with 75% of these
women among other mental health conditions remaining untreated, the need to
identify risk factors and preventable causes increases as a measure to mitigate
the risk of maternal complications and maternal mortality due to suicide33.
Economic stability plays a major role in defining perinatal health. Social determinants such as poverty, being a single parent and refugee status amongst others increase social disparity between low-to-middle income countries and high-income countries34. Specifically, families under these conditions lack financial resources and increased maternal stress that culminates in the form of depressive symptoms and in turn, place infants and toddlers at increased risk of delayed development, leading to a variety of new challenges35. Oftentimes, single parenthood and families of refugee statuses have also been found to be correlated with elevated depression levels, with single mothers at a heightened risk, due to financial difficulties and inadequate social support36. The multifaceted nature of economic instability and its effects, with the added burden of responsibility of supporting a child financially, leads to a perpetuating cycle of maternal mental health issues. Studies from developing countries indicated higher rates of anxiety and depression than those in the United States, those of which connect back to poor infant nutritional status, diarrhea and respiratory illness due to lack of trained staff, funding barriers and affordable medications37.
Social stigma on mental health generally aids in the downplaying of maternal mental health conditions, facing discrimination or prejudice and denial from infant care, leading to self-applied negative or judgmental attitudes that lead to societal withdrawal and increased family financial burdens38. Societal withdrawal, the pattern of reduced social interaction and engagement, is typically associated with shame and fear of reflection and can manifest in avoiding interactions with family members, friends and even healthcare providers, as mothers fear being judged or misunderstood. This isolation exacerbates the financial and emotional burdens on the family, as mothers may also struggle to share the weight of their challenges. The societal rejection of mental health issues, along with the absence of adequate treatment options, can lead to a vicious cycle that is difficult to break.
Culture plays a major role in shaping perceptions of mental health, beginning with public stereotypes and prejudices that develop into self and structured types of stigma that lead to long-term, harmful effects39. Public stereotypes and availability of treatment do also vary across the world. In the 148 countries classified as “developed,” while there are increased statistics of the number of people reporting mental health conditions, mental health and therapy has become less stigmatized and a shift has become much more apparent in recent years40. On the other hand, many Eastern cultures value self-control and conformity, with mental illnesses seen as shameful and generally viewed as a weakness41. In countries or families shaped by these cultural values and perceptions, mothers face more difficulty in confiding in family, seeking out care and/or applying these public stereotypes to themselves. This leads to continued mental health disorders and progression into suicidal thoughts, constantly exacerbating mental health issues and potentially even causing issues in mother-child bonding and attachment, unhealthy for both mother and child.
Maternal health issues can hinder mother-child bonding by affecting the mother’s ability to be responsive and engaged or can lead to decreased sensitivity and caregiving from mother-to-child and increased irritability42. A review done in 2023 highlighted 133 studies that related bonding problems with depression, anxiety and stress showing correlations of 27%, 47% and 27% respectively43. This led them to conclude that maternal psychological distress is associated with postpartum mother-infant bonding, the mother’s emotional response to her infant44.
Poor mental health education is another factor that can lead to perpetual self-isolation or mental health issues due to lack of knowledge of management, hormonal fluctuations before, during and after pregnancy and awareness of the indications of mental health issues as a symptom beyond pregnancy45. It becomes hard for mothers to understand what healthy emotional reactions look like during such a transitional period of time38. Most mental health resources typically have to be individually sought out, but women can also have mental health conversations with OBGYNs. The American College of Obstetricians & Gynecologists recommends that everyone receiving pregnancy care in any capacity be screened for depression and anxiety multiple times but it is not required; rather, providers may ask questions about patient well-being and mothers are encouraged to have those conversations to be able to learn and gather more resources46.
However, in a study done, women with pre-diagnosed moderate-to-severe depression were more likely to accept antidepressants as an acceptable treatment than those without or with minor symptoms. With this, only 44% of African American women, 68% White and 61% Hispanic women among the 73 women in America recruited for this study believed therapy to be an acceptable treatment for depression, contributing to both stigma and the “wait-and-see” method instead of seeking timely treatment, even when it came to OBGYN or other maternal care appointments47.
Social perspectives towards race and gender aren’t exclusive either. Misogny, defined as acts of contempt towards women typically exhibited by men and racism, the belief that race is a fundamental determinant in human capabilities, also contribute negatively to lack of access to care and increased levels of stigma and judgment. Beliefs like these play an important role in heightening barriers of mental health care and highlight the wide range of social determinants that affect perinatal health34.
From a cultural standpoint, different cultures also have unique approaches to maternal health. The Nigerian practice of Omugwo is a postnatal support system that involves elderly women, often the new mother’s mother or mother-in-law, providing assistance in childcare and maternal recovery48. Omugwo serves as a socio-cultural mechanism that helps alleviate postpartum depression (PPD) by reducing maternal stress and fostering emotional support. In contrast, many Western healthcare models emphasize biomedical interventions, with limited integration of extended family support systems49. Research has shown that postpartum depression rates vary widely based on cultural factors, with Nigeria reporting rates around 36.5%, while prevalence in some low-income countries can reach up to 57%50.
In many Asian cultures, traditional postpartum confinement practices, such as "zuo yuezi" in China or "Jaapa" in South Asia, dictate strict dietary and behavioral restrictions for new mothers to ensure proper recovery [51]. While these practices, which include eating nutritious work and avoiding physical overexertion, are believed to protect maternal health, they can also discourage the use of modern healthcare services such as dental care and promote social isolation of the mother due to medical concerns51. A systematic review of 74 studies on traditional maternal practices in Asia found that women often prefer traditional birth positions and avoid hospital births due to concerns about medicalized childbirth experiences52. Healthcare providers working with immigrant populations must recognize these beliefs to provide culturally competent care that aligns with patients’ expectations while ensuring medical safety.
The utilization of formal maternal healthcare also differs among immigrant populations due to language barriers, financial constraints and distrust in unfamiliar medical systems1. For example, studies have shown that immigrant women in high-income countries experience disparities in maternal health outcomes, often receiving inadequate prenatal care due to systemic barriers53. Additionally, the integration of traditional and biomedical healthcare models remains a challenge, as Western medicine prioritizes standardized medical interventions over individualized cultural approaches to childbirth.
2.4.
Special populations & Unique challenges
Pregnancy
is a major developmental change that has a holistic impact on a woman’s
biological, psychological and social
being. The major stage in a woman’s
life can be extremely
stressful, often filled with physical exhaustion, sleep deprivation and poor
financial resources54. For some
women, the level of stress and obstacles are beyond what they can handle based
on their current circumstances. Populations who may be more prone to PDD due to pre-existing
adversity and hardships, such as decreased financial resources, sleep
deprivation and social isolation, include adolescent mothers, incarcerated
mothers and disabled mothers54.
Adolescent mothers are said to be more prone to PPD than adults, where adolescent PPD rates fall between 15% and 50%, as opposed to adult rates of 10%55. Many factors specific to adolescents play a role in this increased vulnerability to depression including persisting cognitive and behavioral developmental changes. Biologically, in situations of heightened emotion and stress, the adolescent brain attenuates the underdeveloped prefrontal cortex, leading to poor judgment and decision-making56. Ill-mannered decisions can end up having an amplified emotional impact on the adolescent, leading to depression. When a precarious situation like pregnancy arises, then they are not only biologically prone to depression, but psychologically as well. Psychological developmental issues root from the inability to reflect and stay in tune with personal emotions regarding delivering a baby57. Social circumstances, like a lack of financial resources and family support, can play a role in harming the mental state of teenage mothers, thus leading to signs of PDD. The vulnerability of teenagers puts them in a situation where a drastic developmental event, like pregnancy, can have crippling effects. Combatting PDD effects in adolescents involves psychotherapies and medications common to adult mothers battling PDD. However, interventions involving greater parent or caregiver involvement will ensure treatment is scheduled and consistent58. This may prove to be a struggle for adolescents facing conflicts with parental relationships following pregnancy, but it is strongly advised to have a trusted adult play a role in the treatment for PDD.
Incarcerated mothers or those imprisoned, are yet another group of women that face greater potential for PDD onset. Many women in jail have predisposing risk factors, like substance abuse disorders, mental health conditions and poverty, which can lead to further complications down the pregnancy timeline59. Complications do not only include the increased likelihood of developing depression perinatally, but also detrimental impacts on the baby. Studies have shown that preterm labor, low birth weight and stillbirth are significant issues that arise with inadequate maternal physical and mental health60. A third of pregnant women in custody in the US are inclined to have elevated stress levels, specifically increasing their chances of not only developing PDD, but other mental health disorders before and during pregnancy61. A contributor to this could be the lack of time spent with the infant post-labor.
Specific aspects of separation between incarcerated mothers and their babies that can lead to the development of PDD include the lack of skin-to-skin contact, along with the inability to breastfeed61. Physical contact is a vital aspect of proper post-labor care, not only for the infant, but also for the mother’s nurturing mental state. Removing that from the post-partum process increases the chances for mothers to feel depressed and detached. The lack of research published on the justice system and maternal health emphasizes the need for better interventions to target specific predisposing factors for perinatal impediments. Disabled mothers are among another population prone to adverse pregnancy outcomes.
Among women with disabilities in the US, 42% report being depressed as opposed to 13% among women without disabilities62. In a study done by health policy researchers in the University of Massachusetts on the depressive symptoms before, during and after pregnancy of disabled and non-disabled women in Rhode Island, 30% of disabled women reported PPD symptoms, as opposed to the 10% of non-disabled women63. Such findings could be attributed to the fact that disabled women face more medical problems, like kidney infections and blood pressure, during pregnancy. The susceptibility roots from the lack of access to proper medical facilities and clinicians who know the proper procedure to treat their specific pregnancy needs.
In addition, women with disabilities may be discouraged to reach out for help due to negative attitudes from healthcare providers and the general public towards disabled women’s capabilities to take the role of a parent64. Additionally, 40% of the disabled women reported being diagnosed with depression prior to pregnancy compared to 16.3% of non-disabled women63. Disabled women inequitably face poor mental health outcomes due to factors like discrimination, ableism, lack of independence and interpersonal violence65. Factors put this specific population in a susceptible position to depression, where a milestone pregnancy can further complicate the mental state of these women. A need for increased psychiatric intervention prior to and during pregnancy is needed to reduce this gap in mental health.
Many groups of women like adolescent mothers, incarcerated mothers and disabled mothers exist outside the typical pregnancy route for mothers. These populations may face increased vulnerabilities to not only PPD, but also hardships before and during the natal period. More research is needed to pursue early intervention and necessary precautions when considering the pregnancy of women who face vulnerabilities prior to beginning this developmental period in life.
2.5.
Screening, diagnosis and treatment
PPD remains
up to 50% underdiagnosed and undertreated due to a lack of using available diagnostic tools and mental
health stigma including having a reluctance to seek help and report symptoms (Figure
1). Standardized universal
screening tools like the Edinburgh
Postnatal Depression Scale (EPDS) and Postpartum Depression
Screening Scale (PDSS) should be used routinely for early detection and
treatment3,66-68.

Figure 1: Edinburgh Postnatal
Depression Scale69.
The EPDS and PDSS both present their own advantages. The EPDS is a free 10-item questionnaire used amongst various ethnic and socioeconomic groups (Figure 1). The PDSS is a lengthier self-report questionnaire that requires purchasing but is more specific as it assesses PPD across sleeping/eating disturbances, anxiety/insecurity, emotional liability, cognitive impairment, loss of self, guilt/shame and contemplating harming oneself70. Despite these differences, both tests are standardized and accurate at screening for PPD68,70.
Pharmacotherapy is one method for treating PPD. Common antidepressants include selective serotonin reuptake inhibitors (SSRIs) like sertraline and fluoxetine, serotonin and norepinephrine reuptake inhibitors (SNRIs) like duloxetine and desvenlafaxine, bupropion and tricyclic antidepressants (TCAs) like amitriptyline or imipramine. Although these drugs did not have an FDA approval for PPD, in 2019, the U.S. Food and Drug Administration (FDA) approved the first drug for treatment of PPD, brexanolone. However, this drug was only approved for intravenous (IV) injection and required health care professions to monitor patients for sedation which limited its use. In August of 2023, the FDA approved zuranolone, the first oral medication for PPD in adults71,72. Brexanolone and zuranolone are novel antidepressants that are allosteric modulators of GABA receptors73. The effects of brexanolone infusion were found as early as within 24 hours of administration74. Similarly, zuranolone was shown to have a rapid-onset and sustained effectiveness for depression with the advantage of it being administered orally73.
Psychological treatments remain an integral part of PPD management. They can be used as either an adjunct to antidepressants or as an alternative for mothers who are hesitant to take medications. Treatments in this category include interpersonal therapies (IPT), cognitive behavioral therapies (CBT), nondirective counseling and peer and partner support. Other nonpharmacologic, non-psychological treatments include acupuncture, massages, electroconvulsive therapies (ECT), bright light therapies, omega-3 fatty acids and exercise75. According to a study by Branquinho et al., CBT was found to be the most effective perinatal treatment despite its modality (such as individual, group, face-to-face or Internet-based)76.
CBT interventions involve identifying thoughts, often those that are catastrophizing, to help change people’s outlook on a situation by replacing previous thoughts with more accurate, positive viewpoints [77]. This is beneficial as it can encourage mothers to seek non-pharmacological treatment if they are reluctant to take antidepressant medications.
2.6.
Analyses of georgia public health data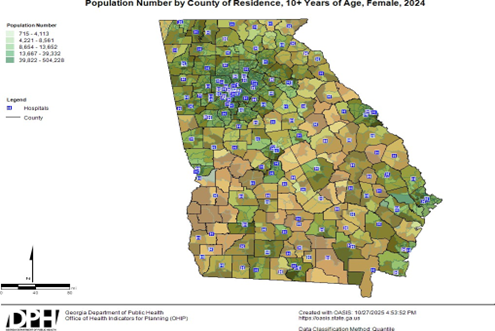
Figure 2: Socioeconomic Vulnerability in Relation to Population of Georgia Counties78.
The map in (Figure 2) from the Georgia Department of Public Health
shows the population density in the state of
Georgia and the socioeconomic vulnerability is overlaid in orange, indicating
which counties have the highest population of women, who fall under the CDC
definition of socioeconomic vulnerability: 150% below poverty, unemployed, no
high school diploma and no health insurance78.
The blue squares indicate hospitals in the county and as seen on the map, there
is a lack of access to care in several rural counties in Georgia which also
overlap with counties with the highest socioeconomic vulnerability. For many
women, this contributes to their risk factors for mental health issues because
there is a lack of access to quality care76,78.

Figure 3: Amount of State Hospitals and Behavioral/Mental Health Facilities by Public Health District30.
The map in (Figure 3) shows the number of mental health care facilities and state hospitals that provide care for mental health concerns in the state of Georgia. As seen above, they are located very far apart and there are very few in rural areas, making them difficult to access30. Additionally, not all of these facilities are appropriately equipped to treat PPD or other mental health related issues and oftentimes patients still need to be referred to another facility, creating further difficulty for patients.
3. Recommendations
3.1. Implement Medicaid reimbursement to pediatric practitioners for screening mothers
for PPD (all but 5 US states
provide reimbursement, with Georgia being one of them)
Postpartum
depression (PPD) is one of the most incapacitating complications of
childbearing and is often neglected
and underdiagnosed79. This underscores the importance of implementing a standardized screening
tool to identify the risk for PPD. According to a study done by researchers at
Purdue University, integrating PPD screening into pediatric primary care
demonstrates improved detection of maternal postpartum depression80. However, screening alone is not
sufficient. Financial incentives and reimbursement structures need to be
implemented to translate screening into a sustained practice. A cohort study in
Colorado found that Medicaid reimbursement for PPD screening for mothers during
well-child visits was associated with a 9.6-percentage point increase in the
probability of having a billed screen for maternal depression81. Similarly, an analysis of a policy change in Michigan, allowing
pediatric providers to bill a child’s Medicaid
ID for PPD screening for mothers during
well-child visits, found that screening rates have increased in recent
years82. In Georgia, the absence
of standardized reimbursement policies and high rates of maternal mental health
challenges makes this type of policy shift vital for improving postpartum care.
3.2. Extend medicaid reimbursement for doula care (efforts to reimburse doula care have been
proposed in Georgia but no action has been taken)
Doulas
are trained individuals that can provide emotional, physical and informational
care to women during pregnancy, delivery and even after childbirth83. Research has shown that community-based
doulas can improve birth outcomes and overall perinatal mental health84. Accessing doula services can be difficult
for families with low socioeconomic status since Georgia
Medicaid does not provide universal care for doula services. A retrospective
cohort study using Medicaid medical claims from California, Florida and a
northeastern state showed that women who received doula care had 52.9% lower
odds of cesarean delivery and 57.5% lower odds of postpartum depression/postpartum anxiety85. These findings suggest
that doulas support safer
delivery outcomes and provide emotional support during the postpartum period.
Therefore, expanding Georgia Medicaid to reimburse doula services can improve overall maternal mental health outcomes.
3.3. Offer paid medical leave during pregnancy (New York is the first state to implement this)
A
lack of national, comprehensive paid medical leave has significant consequences
for pregnant women, especially for those who come from a low-income background86. Pregnant women often face the difficult
balance of prioritizing their own health and maintaining financial stability. Time off from work can mean lost wages or even a risk to job security. Policy makers in New York addressed this challenge by
implementing a law that allows any privately-employed pregnant New Yorkers to
receive an additional 20 hours of paid sick leave for prenatal care in addition
to their existing sick leave87.
Implementing a similar policy in Georgia can help reduce preventable pregnancy
complications and support maternal mental health, which is critical as Georgia has one of the highest
pregnancy-related death rates in the nation88.
4.
Conclusions
Maternal mental
health remains a pressing health
issue all across
Georgia. It is imperative
to address barriers to care for maternal mental health as the number of
postnatal women in Georgia that have reported feelings of depression and
hopelessness have increased in recent years. Postpartum depression (PPD) is
significantly underdiagnosed and understudied. This project highlights how
cultural influences, risk factors and treatment options shape postpartum mental
health outcomes across global contexts. By contrasting biomedical interventions prevalent in Western healthcare models
with familial support systems central to postpartum care in Nigeria and Asian
countries, we can understand key disparities in maternal mental health
outcomes. It is imperative to destigmatize biomedical interventions as well as
ensure cultural sensitivity in maternal mental healthcare. Risk factors for PPD
are multifaceted and include trauma during birth, prior mental illness, lack of
social support and financial constraints. Since these factors often delay
diagnosis and limit access to perinatal care, we must utilize standardized universal screening tools
such as Edinburgh Postnatal Depression Scale (EPDS) or Postpartum Depression
Screening Scale (PDSS) for early detection of PPD. By pairing these screening
tools with pharmacological treatments, such as zuranolone and brexanolone and
psychological treatments, such as interpersonal therapies (IPT) and cognitive
behavioral therapies (CBT), we can improve PPD diagnosis and maternal mental
health outcomes globally.
5.
References
- Zaidi M, Fantasia HC, Penders R, et al. Increasing U.S. maternal health equity among immigrant populations through community engagement. Nursing for Women’s Health, 2024;28: 11-22.
- World Health Organization (WHO). Perinatal Mental Health. World Health Organization,
2025.
- Carlson K, Mughal S, Azhar Y, et
al. Perinatal Depression. InStatPearls. StatPearls, 2025.
- Agrawal I, Mehendale AM, Malhotra R. Risk factors of postpartum
depression. Cureus, 2022.
- Place JM, Renbarger K, Van De Griend K, et
al. Barriers to help-seeking for postpartum depression mapped onto the
socio-ecological model and recommendations to address barriers. Frontiers in Global
Women’s Health, 2024;5.
- Halbreich U, Karkun S. Cross-cultural and social diversity of prevalence of
postpartum depression and depressive symptoms. Journal of Affective Disorders,
2006;91: 97-111.
- Chen C, Okubo R, Okawa S, et
al. The prevalence and risk factors of suicidal ideation in women
with and without postpartum depression. Journal of Affective Disorders, 2023;340:
427-434.
- Payne JL, Maguire J. Pathophysiological mechanisms implicated in
postpartum depression. Frontiers in Neuroendocrinology, 2019;52: 165-180.
- American Psychological Association. Postpartum depression: Causes, symptoms,
risk factors and treatment options. American Psychological Association, 2022.
- Tang L, Zhang X, Zhu R. What causes postpartum depression and how to
cope with it: A phenomenological study of mothers in China. Health
Communication, 2020;36: 1495-1504.
- Callister LC, Beckstrand RL, Corbett C. Postpartum depression and
help‐seeking
behaviors in immigrant Hispanic women. Journal of Obstetric, Gynecologic & Neonatal Nursing, 2011;40: 440-449.
- US.
Department of Health & Human Services, Health Resources & Services
Administration. III.C. Needs Assessment Update - Georgia, 2024.
- Amnesty International. Deadly delivery: The maternal health care crisis in the
USA (Index AMR 51/007/2010). London, United Kingdom: Amnesty International,
2010.
- Hagatulah N,
Bränn E, Oberg AS, et al. Perinatal depression and risk of mortality: Nationwide, register-based study in
Sweden. BMJ, 2024;384: 075462.
- March of Dimes. Nowhere to go: Maternity care deserts across the US,
2024.
- Habel C, Feeley N, Hayton B, et
al. Causes of women׳s postpartum depression symptoms:
Men’s and women׳s perceptions. Midwifery, 2015;31: 728-734.
- Rodrigues M,
Patel V, Jaswal S, et al. Listening to mothers: Qualitative studies on
motherhood and depression from Goa, India. Social Science & Medicine, 2003;57:
1797-1806.
- Guintivano J, Arad M, Gould TD, et
al. Antenatal prediction of postpartum depression with blood DNA methylation biomarkers. Molecular
Psychiatry, 2013;19: 560-567.
- Mayo
Foundation for Medical Education and Research. Postpartum depression: Symptoms
and causes. Mayo Clinic, 2018.
- Raza SK,
Raza S. Postpartum Psychosis. In: StatPearls. Treasure Island (FL): StatPearls, 2025.
- Friedman SH, Reed E, Ross NE. Postpartum psychosis. Current
Psychiatry Reports, 2023;25: 65-72.
- Friedman SH, Sorrentino R. Commentary: postpartum psychosis, infanticide
and insanity-implications for forensic psychiatry. The Journal of the
American Academy of Psychiatry and the Law, 2012;40: 326-332.
Charatan F. Mother who drowned her five children is granted a retrial after witness gave false evidence. BMJ, 2005;330. - Alipour Z, Kheirabadi GR, Kazemi A, et
al. The most important risk factors affecting mental health
during pregnancy: A systematic review. Eastern Mediterranean Health Journal, 2018;24: 549-559.
- Lansford
JE. Annual Research Review: Cross-cultural similarities and
differences in parenting. Journal of Child Psychology and Psychiatry
and Allied Disciplines, 2022;63: 466-479.
- Bashiri N, Spielvogel AM. Postpartum depression: A cross-cultural
perspective. Primary Care Update for OB/GYNS, 1999;6: 82-87.
- Wang Z, Liu J, Shuai H, et
al. Mapping global prevalence of depression among postpartum women.
Translational Psychiatry, 2021;11.
- Vuncannon
DM, Dunlop AL, Platner MH, et al. 707 patient factors associated with severe maternal
morbidity by urban-rural designation in Georgia, United States. American
Journal of Obstetrics and Gynecology, 2024;230.
- Miteniece
E, Pavlova M, Shengelia L, et al. Barriers to accessing adequate maternal care in Georgia: A qualitative study. BMC Health Services
Research, 2018;18: 631.
- DBHDD, Office of Decision Support. Georgia Department of Behavioral
Health & Developmental Disabilities Regional Map with Community Service
Areas Effective July 1, 2020 [Review of Georgia Department of Behavioral Health
& Developmental Disabilities Regional Map with Community Service Areas
Effective July 1, 2020]. Georgia Department of Behavioral Health and
Developmental Disabilities, 2021.
- Grisbrook MA, Dewey D, Cuthbert C, et
al. Associations among Caesarean Section Birth, Post-Traumatic Stress and
Postpartum Depression Symptoms. International Journal of Environmental Research
and Public Health, 2022;19: 4900.
- Zedan HS, Baattaiah
BA, Alashmali S, et al. Risk of postpartum depression: The considerable role of maternal health status and lifestyle.
Healthcare, 2023;11: 2074.
- Byatt
N, Levin LL, Ziedonis D, et al. Enhancing Participation in Depression Care in Outpatient Perinatal Care Settings: A
Systematic Review. Obstetrics and Gynecology, 2015;126: 1048-1058.
- Vora SJ, Ebenezar A, Chaitanya B, et
al. Comparison of Outcomes of Non-diffractive Extended Depth of
Focus Intraocular Lens and Diffractive Extended Depth of Focus Intraocular
Lens. Cureus, 2025;17: 91413.
- Beeber LS, Perreira KM, Schwartz T. Supporting the Mental Health of
Mothers Raising Children in Poverty. Annals of the New York Academy of
Sciences, 2008;1136: 86-100.
- Kareem OM, Oduoye MO, Bhattacharjee P, et
al. Single parenthood and depression: A thorough review of current
understanding. Health Science Reports, 2024;7: 2235.
- Ghaffar A, Langlois EV, Rasanathan K, et al. Strengthening health systems through embedded research. Bulletin of the World
Health Organization, 2017;95: 87.
- Pokhrel
A, Virk S, Snider JL, et al. Estimating yield-contributing physiological parameters of cotton using UAV-based imagery. Frontiers in Plant Science,
2023;14.
- Singhal N. Stigma, prejudice and discrimination against people with
mental illness. American Psychiatric Association, 2024.
- Convit J. Mental health in developed vs developing countries |
Jacinto Convit World Organization. Jacinto Convit, 2021.
- Birtel MD, Mitchell BL. Cross‐cultural differences in depression between White
British and South Asians: Causal attributions, stigma by association,
discriminatory potential. Psychology and Psychotherapy: Theory, Research and Practice,
2022;96.
- La Rosa VL, Alparone D, Commodari E. Psychological and social factors
influencing mother–child bonding in the first year after birth: A model for
promoting infant and maternal well-being. Frontiers in Psychology, 2025;16.
- O’Dea
GA, Youssef G, Hagg L, et al. Associations between maternal psychological distress and mother-infant bonding:
a systematic review and meta-analysis. Archives of Women’s Mental Health,
2023;26(4).
- Condon JT, Corkindale CJ. The assessment of parent-to-infant attachment:
Development of a self-report questionnaire instrument. Journal of Reproductive
and Infant Psychology, 1998;16: 57-76.
- Highet NJ, Gemmill AW, Milgrom J. Depression in the perinatal period:
Awareness, attitudes and knowledge in the Australian population. The Australian
and New Zealand Journal of Psychiatry, 2011;45: 223-231.
- ACOG.
Patient screening, 2025.
- Sleath B, Blalock SJ, Carpenter DM, et
al. Ophthalmologist-patient communication, self-efficacy and glaucoma medication
adherence. Ophthalmology, 2015;122: 748-754.
- Iwuagwu
AO. “Ọmụgwọ” as unpaid labor? The perceptions of postpartum caregiving among older grandmothers in Southeast Nigeria. Innovation in Aging, 2023;8.
- Howard LM, Khalifeh H. Perinatal Mental Health: A Review of Progress
and challenges. World Psychiatry, 2020;19: 313-327.
- Adeyemo EO, Oluwole EO, Kanma-Okafor OJ, et
al. Prevalence and predictors of postpartum depression among postnatal women in
Lagos, Nigeria. Afr Health Sci, 2020: 1943-1954.
- Raven JH, Chen
Q, Tolhurst RJ, et al. Traditional beliefs and practices in the postpartum period in Fujian Province, China: A qualitative study. BMC
pregnancy and childbirth, 2007;7: 8.
- Withers
M, Kharazmi N, Lim E. Traditional beliefs and practices in pregnancy, childbirth and postpartum: A review of the evidence from Asian countries.
Midwifery, 2018;56: 158-170.
- Eslier M, Azria E, Chatzistergiou K, et
al. Association between migration and severe maternal outcomes in high-income
countries: Systematic review and meta-analysis. PLoS medicine, 2023;20:
1004257.
- Ladores S, Corcoran J. Investigating postpartum depression in the adolescent
mother using 3 potential qualitative approaches. Clinical Medicine Insights:
Pediatrics, 2019;13.
- Kingston
D, Heaman M, Fell D, et al. Comparison of adolescent, Young Adult and adult women’s maternity experiences and practices. Pediatrics, 2012;129.
- Spear LP. Adolescent Neurodevelopment. Journal of Adolescent Health, 2013;52:
7-13.
- Sadler LS, Novick G, Meadows-Oliver M. Having a baby changes everything reflective functioning in pregnant adolescents. Journal of Pediatric Nursing,
2016;31.
- Grover S, Avasthi A. Clinical Practice Guidelines for the management of
depression in children and adolescents. Indian Journal of Psychiatry, 2019;61,
226-240.
- Kramer
C, Bradley D, Shlafer RJ, et al. Maternal health and incarceration: Advancing pregnancy justice through research. Health & Justice,
2025;13.
- Bard E, Knight M, Plugge E. Perinatal health care services for imprisoned
pregnant women and associated outcomes: a systematic review. BMC Pregnancy
Childbirth, 2016;16: 285.
- Chawla A, Bansal NL, Liu C, et
al. Postpartum depression in correctional populations. Journal
of Correctional Health Care, 2024.
- CDC. Disability and Health Data. Centers for Disease Control and Prevention,
2018.
- Mitra M, Iezzoni LI, Zhang J, et
al. Prevalence and Risk Factors for Postpartum Depression Symptoms Among Women
with Disabilities. Maternal and Child Health Journal, 2014;19: 362-372.
- Signore C, Davis M,
Tingen CM, et al. The intersection of disability and pregnancy: Risks for maternal morbidity and mortality. Journal of Women’s
Health, 2021;30: 147-153.
- Deierlein AL, Park C, Patel N, et
al. Mental health outcomes across the reproductive life course among
women with disabilities: a systematic review. Archives of Women’s Mental
Health, 2024.
- Carrel-Lammert M, Holbert M, Devaiah G, et
al. Universal early postpartum depression screening in the inpatient
postpartum unit: An opportunity for early intervention. American Journal of
Obstetrics and Gynecology, 2022;226.
- Manso-Córdoba S,
Pickering S ortega MA, et al. Factors related to seeking help for postpartum depression: A secondary analysis of New
York City PRAMS data. International Journal of Environmental Research and
Public Health, 2020;17: 9328.
- MGH Center for Women's Mental Health. Identifying postpartum
depression: A three question screening tool, 2008.
- Cox JL, Holden JM, Sagovsky R. Edinburgh Postnatal Depression Scale
(EPDS) [Database record]. APA PsycTests, 1987.
- Chaudron LH, Szilagyi PG, Tang W, et
al. Accuracy of depression screening tools for identifying postpartum
depression among urban mothers. Pediatrics, 2010;125: 609-617.
- US Food and Drug Administration. FDA approves first oral treatment
for postpartum depression, 2023.
- US Food and Drug Administration. FDA approves first treatment for
post-partum depression, 2019.
- Qiu Y, Tao Y, Duan A, et
al. Efficacy and tolerability of zuranolone in patients with depression: a
meta-analysis of randomized controlled trials. Frontiers in pharmacology, 2024;14: 1334694.
- Zheng W, Cai D-B, Zheng W, et
al. Brexanolone for postpartum depression: A meta-analysis of randomized controlled studies. Psychiatry Research, 2019;279: 83-89.
- Fitelson
E, Kim S, Baker AS, et al. Treatment of postpartum depression: clinical, psychological and pharmacological options. International journal of
women's health, 2010;3: 1-14.
- Branquinho M, Rodriguez-Muñoz M, de la
F, et al. Effectiveness of psychological interventions in the treatment of perinatal depression: A
systematic review of systematic reviews and meta-analyses. Journal of Affective
Disorders, 2021;291: 294-306.
- Basson R, Bronner G. Management and rehabilitation of neurologic patients
with sexual dysfunction. In D. B. Vodušek & F. Boller (Eds.), Handbook of
clinical neurology, 2015;130: 415-434. Elsevier.
- Georgia Department of Public Health, Office of Health Indicators for Planning - OASIS.
- Khamidullina Z, Marat
A, Muratbekova S, et al. Postpartum depression epidemiology,
risk factors, diagnosis and management: An appraisal of the current knowledge
and future perspectives. Journal of Clinical Medicine, 2025;14: 2418.
- Sorg
M, Coddington J, Ahmed A, et al. Improving postpartum depression screening in pediatric primary care: A quality improvement project. Journal of
Pediatric Nursing, 2019;46: 83-88.
- Gordon SH, Lee S, Deen N, et
al. Medicaid reimbursement for maternal depression screening and care for postpartum
depression. JAMA Pediatrics, 2025;179: 1009.
- Currie J, Malinovskaya A. Screening for postpartum depression at well child
visits: Evaluating the impact of Michigan’s statewide initiative. Health
Economics Review, 2025;15.
- Horan HL. Doula support as a health equity strategy: Carving the path forward.
American Journal of Public Health, 2024;114: 1161-1163.
- Davenport SC, Corlette S, Davenport K, et
al. Doula Medicaid reimbursement by State. Center For Children and Families,
2025.
- Falconi AM, Burt SB, Tang
T, et al. Doula care across the maternity care continuum and impact on Maternal
Health: Evaluation of Doula programs across three states using propensity score matching. SSRN
Electronic Journal, 2022.
- Garner A. Paid family medical leave remains critical for low-income pregnant
and postpartum women. 1,000 Days, 2022.
- Schreider
C. New York enacts paid prenatal personal leave. Crowell & Moring - New
York Enacts Paid Prenatal Personal Leave, 2024.
- Kondracki AJ, Li W, Mokhtari M, et al. Pregnancy-related maternal mortality in the state of Georgia: Timing and causes
of death. Women’s Health, 2024;20.