A Case of 25-Year-Old-HIV-Infected Male with Acute Pericarditis
Abstract
A cute pericarditis is defined as inflammation of the pericardium that surrounds the heart and the base of the great vessels. The classical presentation consists of chest pain, a pericardial friction rub and serial changes on electrocardiogram. We report a case of typical acute pericarditis in a 25-year-old male with hiv infection.
Keywords: pericarditis; hiv infection
1. Introduction
A cute pericarditis is defined as inflammation of the pericardium that surrounds the heart and the base of the great vessels. The classical presentation consists of chest pain, a pericardial friction rub, and serial changes on electrocardiogram. Although data on the incidence of pericarditis are lacking, estimates indicate that it is the cause of at least 1% of emergency room visits among patients with st-segment elevation and up to 5% of emergency room visits for nonischemic chest pain1,2. The main pericardial syndromes encompass pericarditis (acute, subacute, chronic, recurrent), pericardial effusion, cardiac tamponade and pericardial masses. Pericarditis is the most common form of pericardial disease worldwide and is typically encountered in young and middle-aged people3. It represents 0.2% of all hospital admissions of cardiovascular aetiology and approximately 5% of patients with nonischaemic aetiology chest pain, presenting in the emergency departments of north america and western europe3. Acute pericarditis is the most common pericardial syndrome in clinical practice.
1.
Case presentation
A
25-year-old male patient was admitted to the hospital because of pericardial
chest pain: sharp pain, increased when breathing deeply and when lying down,
decreased when sitting and bending forward. Past history of hiv infection. On
review of systems, the patient reported no fever, chills, malaise, and a
headache. He denied sore throat, nasal congestion, body aches, cough or ear
pain. Further evaluation of the patient revealed the following vital signs: t
37°c blood pressure 120/60 mmhg pulse 101 bpm respiratory rate 16 o2
sat 97% he did not appear toxic and his exam was normal. A rapid flu test was
negative. His ecg (figure 1) demonstrated diffuse concave-upward
st-segment elevation and pr-segment depression, st-segment depression in avr or
v1. The patient’s chest x-ray (figure 2) showed an normal heart. Given
the patient’s history and clinical findings, he was referred to the emergency
room for suspected pericarditis with pericardial effusion.
2.
Discussion
Although
viral infection is the most common identifiable cause of acute pericarditis,
there are multiple other etiologies, as listed in (table 1). The classic
history of acute pericarditis begins with prodromal symptoms of fever, myalgia,
and malaise. It is followed by acute onset of pleuritic, substernal chest pain
that may radiate to the scapular ridge, neck, arms or jaw. The pain is usually
relieved by leaning forward and made worse with laying supine4. Other associated symptoms include low-grade
intermittent fever, dyspnea, tachypnea, cough and dysphagia. A pericardial
friction rub is the most specific physical exam finding in pericarditis
(specificity approaching 100%), however, this exam finding is transient over
time, has a low sensitivity, and may be present in only about 50% of cases4,5. The rub is best heard over the left sterna
border, during expiration with the patient leaning forward. It is characterized
by a grating or rasping sound similar to leather rubbing together4,6. A major life-threatening complication of
acute pericarditis is cardiac tamponade. Pericardial effusion results from
accumulation of fluid between the visceral and parietal layer of the
pericardium. Tamponade occurs when the fluid pressure in the intrapericardial
space alters cardiac filling. The classic signs as described by beck’s triad
are hypotension, jugular venous distension, and muffled heart sounds. Another
important physical exam finding is pulsus paradoxus, a drop of at least 10 mmhg
in arterial blood pressure on inspiration4,6.
Cardiac tamponade is a medical emergency and patients should be transferred to
an emergency care setting for further evaluation. During acute pericarditis,
ecg changes evolve through four stages as described in (table 2)4,6-8. The hallmark ecg findings of diffusely
concave upward st elevation (not seen in v1 and avr) with upright t waves, and
a pr interval that deviates opposite of the p wave polarity are found during
stage i (figure 1). Chest x-ray is usually normal in patients with
pericarditis and minimal effusion. However, when a large amount of effusion is
present (200- 250 ml), a chest x-ray will reveal a flask-shaped, enlarged
cardiac silhouette, and a possible left-sided pleural effusion7. The chest x-ray taken of our patient
demonstrated an normal cardiac silhouette. In this case, an echocardiogram
would be warranted to further evaluate the significance of the effusion and
assess cardiac function and there was no pericardial effusion. High sensivity
cardiac troponin i were negative 2 times 3 hours apart.
2.1
Diagnosis
Presumed
viral (hiv) pericarditis. Treatment for pericarditis is directed toward the
underlying cause. For idiopathic and viral pericarditis, therapy should be
directed toward symptom control. Nonsteroidal anti-inflammatory drugs (nsaids)
are the mainstay of therapy6.
Colchicine is a useful adjunct to nsaids and was once reserved for patient with
recurrent or prolonged symptoms5.
Data from the colchicine for acute pericarditis trial has led to its routine
use by many practioners6.
Corticosteroids are not recommended for first-line treatment unless indicated
for the underlying disease or because of lack of response to nsaids or
colchicine6. Nsaids and
steroids should not be used in pericarditis associated with acute myocardial
infarction (mi). Pericardiocentesis is indicated when significant pericardial
effusion is present, for both diagnostic and therapeutic purposes.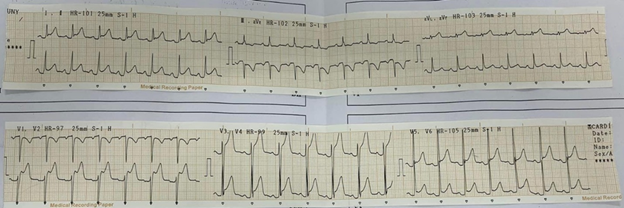
Figure 1. Ecg show diffuse concave-upward st-segment elevation and pr-segment
depression, st-segment depression in avr or v1.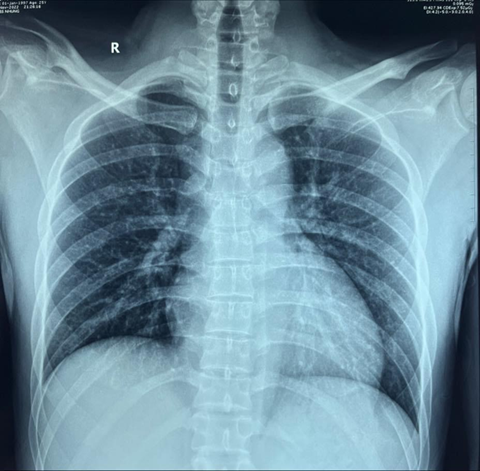
Figure 2. Chest xray showed normal
Table 1. Main causes of acute pericarditis3
|
Categories |
Causes |
Frequency |
|
A. Idiopathic |
Unknown |
Most frequent cause |
|
b. Infectious causes |
|
|
|
Viral |
Epstein-barr, influenza, hepatitis, human immunodeficiency virus,
mumps, echovirus, adenovirus, cytomegalovirus, varicella, rubella, human
herpesvirus, parvovirus, coxsackie |
Most frequent cause in developed countries |
|
Bacterial |
Mycobacterium tuberculosis, coxiella burnetii, streptococcus,
staphylococcus, pneumococcus, legionella, salmonella, haemophilus |
Rare (with the exception of mycobacterium tuberculosis) |
|
Fungal |
Candida, aspergillosis, histoplasmosis, blastomycosis |
Very rare |
|
Parasitic |
Toxoplasma, echinococcus |
Very rare |
|
c. Non-infectious causes |
|
|
|
Neoplastic |
Primary: pericardial mesothelioma |
Frequent as secondary metastasis |
|
Secondary tumours: leukemia, breast cancer, lung cancer, |
||
|
Lymphoma, melanoma |
||
|
Metabolic |
Hypothyroidism, renal failure, hypercholesterolaemia, gout, anorexia
nervosa |
Frequent |
|
Cardiovascular |
Acute myocardial infarction, dressler's syndrome, aortic dissection |
Frequent |
|
autoimmune |
Rheumatoid arthritis, systemic lupus erythematosus, sjogren syndrome,
dermatomyositis, sarcoidosis, systemic vasculitides, behçet's syndrome,
familial mediterranean fever |
Frequent |
|
Traumatic and iatrogenic |
Catheterisation, surgery, chest trauma, radiation |
Frequent |
|
Drug-related |
Phenytoin, minoxidil, isoniazid, procainamide, hydralazine,
methyldopa, doxorubicin, amiodarone, clozapine, streptomycin |
Rare |
|
Other |
Congenital absence of pericardium |
Rare |
Table 2. Stages of ecg changes during acute pericarditis3,4
|
Stage i: hallmark signs. Occurs in early stages of disease. Includes diffuse
concave upward st elevation, elevation not seen in leads avr and v1, t waves
are upright in the leads with st Segment elevation,
and pr segment deviates opposite of p wave polarity. Stage ii: occurs several days after onset of symptoms. St segment return to
baseline. And t waves flatten. Stage iii: t waves become inverted. No q waves should be seen. Stage iv: weeks to months. Ekg normalizes or if chronic pericarditis develops,
t wave inversions may remain indefinitely
|
1.
Conclusion
This case highlights several important issues
for urgent care providers. First is the danger of “anchoring” to the diagnosis
of a prior provider. All patients presenting to urgent care deserve a full
investigation of their chief complaint with an open mind as to the cause. The
clinical presentation of the patient in this case warranted further
investigation to rule out other significant disease processes, such as mi and
pulmonary embolism. The second important issue is that medical conditions are
dynamic and evolve. While it may be tempting to criticize the first provider
for having “missed” the diagnosis, we do not know if the key features of sharp
positional chest pain, tachycardia were present 4 days prior. A third key issue
is to make sure the clinical presentation is consistent with the patient’s
diagnosis. Several features make this case inconsistent with the original
diagnosis of upper respiratory infection. The presence of positional pleuritic
chest pain and subtle vital sign abnormalities and the absence of upper
respiratory infection symptoms warranted the chest x-ray and ecg, which made
the diagnosis obvious.
2.
Author contributions
The author wrote the
manuscript. The author have read, reviewed, and approved the article.
3.
Funding
No funding was received for this article.
4.
Availability of data and materials
The datasets used during the current study
are available from the corresponding author on reasonable request.
5.
Declarations
Ethics approval and consent
to participate
This study was performed in accordance with
the declaration of helsinki. The patient gave informed consent, and the
patient’s anonymity was preserved.
Consent for publication
Written informed consent for publication was
obtained from the patient for publication of this case report and any
accompanying images. A copy of the written consent is available for review by
the editor-in-chief of this journal.
6.
Competing interests
The author declare that they have no
competing interests.
References
2. Troughton rw, asher cr, klein al.
Pericarditis. Lancet 2004;363:717-727.
4. Tingle te, molina d, calvert cw. Acute
pericarditis. Am fam physician 2007;76(10):1509-1514.
5. Spodick dh. Acute pericarditis: current
concepts and practice. Jama 2003;289(9):1150-1153.
6. Little wc, freeman gl. Pericardial
disease. Circulation. 2006;113(12):1622-1632.
7. Goyle kk, walling ad. Diagnosing
pericarditis. Am fam physician 2002;66(9):1695-1702.