A Case of Fourth Branchial Cleft Anomaly
ABSTRACT
A rare source of lateral neck masses of congenital
origin are branchial abnormalities, which arise from aberrant development
during embryogenesis. The most frequent source of origin is the second
branchial cleft; anomalies resulting from the first, third, and fourth clefts
are less common. Even though branchial cleft-derived cysts are rare, it's
crucial to take this condition into account when making a differential
diagnosis for neck masses, especially those that are laterally situated. This
article presents the rare case of a child of 6 years who presented the sudden
appearance of a lateral collection in the neck fistulized to the skin with
notion of recurrent neck infections at the same site. patient underwent
extensive diagnostic examinations, including radiology, which were consistent
with a left subcutaneous collection measuring17.2*15 mm with irregular,
heterogeneous and hypoechogenic contours. A 5 centimeter sinus that descends to
the thoracic orifice from the internal jugular vein and the common carotid
artery was discovered during the cervicotomy. After resectioning it, each sinus
extremity had 3.0 resorbable sutures placed. To guarantee complete closure of
the sinus, a piece of sternocleidomastoid muscle was inserted. Nine months
following the surgery, there were no signs of a neck infection or purulent
episode. This clinical example highlights how critical it is to identify
uncommon illnesses like branchial cleft cysts as soon as possible and treat
them appropriately.
Keywords: Branchial
apparatus; Branchial cyst; Branchial cleft anomaly
INTRODUCTION
During the fourth week of pregnancy, the gill
apparatus, also known as the branchial arches, which are made up of endodermal
pouches and ectodermal clefts, aid in the correct development of the head and
neck. Incomplete obliteration causes congenital malformations of the ectodermal
clefts of the branchial arches, which in most cases (75%) culminate in a cyst
and in 25% in a sinus1.
Roughly 17% of all pediatric neck masses are
abnormalities related to branchial clefts2.
These are typical congenital lesions that are typically identified in the early
years of life in children3. A cyst,
sinus, or fistula may occur as a result of a branchial apparatus failing to
involutate4. Less than 1% of
branchial anomalies are fourth branchial arch anomalies, which primarily affect
the left side and manifest as suppurative thyroiditis or recurrent neck
infections5.
Cysts with a fourth branchial cleft parallel to the
recurrent laryngeal nerve are extremely rare. Like third branchial cleft
sinuses, they are most frequently found on the left side (80%), and they
typically form a sinus that extends from the apex of the piriform sinus.
However, instead of passing superiorly to reach the anterior left upper thyroid
lobe, they travel inferiorly. Cysts can occur anywhere in the neck, all the way
down to the mediastinum, but they are typically found next to the thyroid gland.
It is challenging to differentiate radiologically between anomalies involving
the third and fourth branchial clefts due to their close closeness. The link
between the sinus tract and the superior laryngeal nerve needs to be surgically
identified in order to provide an appropriate diagnosis.
CASE PRESENTATION
We report the case of a 6-year-old girl, presenting
for 2 years with a left cervical latero tumor fistulized at the skin, treated
with antibiotics (amoxicilin and clavulanic acid) with a recurrent history of
infections and abscesses of the neck, 2 biopsies were made which were not
significant. a cervical ultrasound was requested revealing the presence of
subcutaneous collection measuring17.2*15 mm with irregular, heterogeneous and
hypoechogenic contours.There were also air bubbles appearing behind the left thyroid
lobe, infront of the left thyroid cartilage when the patient was performing
Vasalva’s maneuver. Patient underwent hypopharyngoscopy revealing the presence
of an orifice of the sinus was found in the left piriform fossa (Figure 1).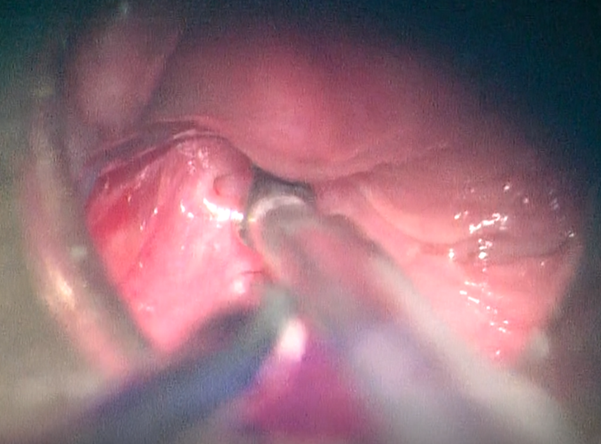
Figure
1. Orifice of the fistula in the left
piriform fossa in endoscopic view.
The Cervicotomy revealed a sinus located between the
common carotid artery and the internal jugular vein. The sinus had pus inside (Figure 2). It was resected and 3.0
absorbable sutures were placed at each end of the sinus. A fragment of
sternocleidomastoid muscle was interposed to ensure complete closure of the
sinus, before closing the planes over a drainage tube. The drainage tube was
removed after 2 days. There were no postoperative events. No suppurative events
or neck infections were noted 6 months after the operation.
DISCUSSION
The branchial arches are the source of certain unique
neck structures. The superior parathyroid glands, the laryngeal cartilages, the
pharyngeal and laryngeal constrictor muscles, the superior laryngeal nerve, the
left thoracic aorta, the proximal right subclavian artery, and the final
branchial body that forms the thyroid's parafollicular cells are all descended
from the fourth branchial arch. The neck structure is altered when the
pharyngobranchial duct and fourth branchial cleft are not completely obliterated6.
Fourth branchial cleft sinuses are a rare condition
with a left side predominance that were initially described by Sandborn and
Shafer in 19727,8. In 105 individuals
who underwent surgery to address branchial anomalies, Li et al. found that 3.7%
of them had fourth branchial cleft anomalies9.
In the pediatric population, they result in deep neck infections10. The 3-year-old child's left side had the
suppurative mass in the instance that was being presented.
Thirty percent of congenital neck masses are branchial
cleft anomalies, of which only two percent are fourth branchial cleft
anomalies, an incredibly unusual occurrence. Anomalies resulting in a fourth
branchial cleft typically show up as cysts in adults and as sinuses or fistulas
in children. The tip of the piriform sinus is where these laryngotracheal sinus
tracts start, and they extend inferiorly to leave the throat through the
lateral cricothyroid membrane. After that, they go inferiorly and might be found
encircling the right subclavian artery or left aortic arch11. (Figure
2).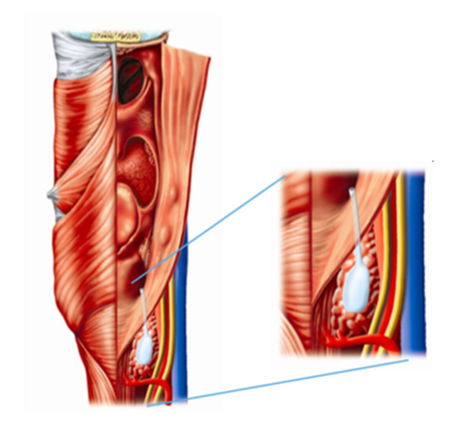
Figure
2. The predicted tract of a fourth
branchial anomaly
The clinical presentation of fourth branchial arch
abnormalities varies with age. The most frequent presenting symptoms in
neonates are dyspnea episodes12.
Cervical cutaneous fistulas appear in childhood, and these cysts later present
classically with a recurrent history of infections and neck abscesses,
typically on the left side in 93.6% of cases, the right side in 6%, and
bilaterally in 0.5% of circumstances. Clinically, infectious episodes manifest
as chronic neck edema. They can also affect the thyroid lobe on the ipsilateral
side of the cyst, resulting in acute suppurative thyroiditis. When these signs
are observed in the neck, subacute de Quervain's thyroiditis, Hashimoto's
thyroiditis, or bleeding from a thyroid nodule should be considered as differential
diagnoses6. 19% of cases of
congenital abnormalities of the fourth branchial arch were found to be
associated with bacterial superinfections as a result of the hypopharynx's
retrograde transmission of flora, which includes anaerobic bacteria like
Eikonella corrodens, Citrobacter, and Proteus as well as a variety of aerobic
microorganisms like Streptococcus, Staphylococcus, Haemophilus, and Escherichia
coli. The review of 526 cases revealed this information13.
Branchial cysts have been investigated using a range
of diagnostic techniques, the most effective of which have been direct
laryngoscopy and barium esophagogram, which have the highest positive
predictive values (between 88% and 90%, respectively). In contrast to
laryngoscopy, barium studies might not reveal a sinuous tract if there is
inflammation. Cystic lesions can also be diagnosed and assessed using other
methods such thyroid ultrasonography, computed tomography, and magnetic
resonance imaging. Numerous anomalies are identified by chance discoveries13.
Treatment options for abscesses of the third and
fourth branchial arches include drainage and incision, which are commonly used
but have a high recurrence rate of up to 90%. Because of the possibility of a
serious infection or primary cancer, surgical excision combined with a partial
thyroidectomy is the suggested course of treatment for cysts, sinuses, and
fistulas14,15. Surgery carries a
higher risk of complications or damage to cervical neurovascular systems,
particularly in infants and neonates, but a decreased likelihood of recurrence12.
After surgery, we discovered a 5 cm long and 1 cm wide
sinus tract that was constrained by the thoracic orifice on his caudal side and
the hypopharynx on his cranial side. Barberet16
described this specific surgical condition and noted that the sinus tract may
terminate on the aortic cross. Before closing the fistulous orifice plan by
plan, a 3.0 absorbable wire was used to pussend the fistula and insert a
fragment of SCM, making the opening blind. On the mentioned orifice, there was
no endoscopic intervention.To repair the fistula and lower the chance of
recurrence, Givens et al. employed a flap of rotation of the sternohyoid muscle16. Numerous writers have referred to pharyngeal
opening fistula closure as the gold standard of therapy to prevent recurrences8,9,17. Peirera et al. also recommend this
modality, associated or not with a loboisthmectomy depending on whether the
thyroid lobe is affected or not18. In
front of a thyroid gland that is macroscopically normal, we did not execute a
loboisthmectomy. Several treatment approaches have been reported, most notably
Watson's, who discovered positive outcomes in five patients undergoing endoscopic
coagulation (thermal by electrocoagulation, chemical with silver
nitrate/trichloroacetic acid, or CO2 laser) of the fistulous orifice7,18,20,21. With 11, 10, and 19 infants treated
with endoscopic cauterization, respectively, Kim, Verret, and Leboulanger have
the biggest series of patients7,20,21.
In these series, the recurrence rate varies from 0% to 35%. Simple incisions
drainage are the primary cause of recurrences, as seen in 94% of cases here17. Recurrence rates with endoscopic
cauterization are 18%, while open surgery without touch on the thyroid has a
15% rate, according to Nicoucar et al. Considering these numbers17.
5% to 6% of patients have been documented to have
surgical site infections, salivary fistulas, and vocal cord paralysis as
consequences following surgical and cauterization operations. Due to
inflammation and edema that may eventually compress these nerves during
electrocautery, paralysis of the superior and recurrent laryngeal nerves may
result. Despite the paucity of evidence, the majority of research come to the
conclusion that cauterization which is less invasive, has a lower risk of
complications, and can be done concurrently with other operations like incision
and drainage in the event of an abscess should be the main course of treatment22,23. Moreover, reports of sclerosing
agent-treated cases that were successful have been published24.
The outcomes of endoscopic surgery are comparable to
those of open surgery, despite the fact that the less invasive endoscopic
approach appears to be favoured these days due to the decreased chance of
laryngeal nerve injury. In their description of a novel endoscopic procedure,
Huang et al. used the KTP laser in conjunction with fibrin glue on five
children without reporting any complications or recurrences8.
CONCLUSION
To sum up, lateral neck tumors can have fourth
branchial cleft anomalies as an uncommon but significant differential
diagnosis. Age-related differences in clinical manifestations are common, and
viral episodes can cause major side effects. A combination of imaging and
direct laryngoscopy is usually used to make the diagnosis. Surgical excision
and partial thyroidectomy are the suggested treatments to lower the risk of
primary cancer and severe infection and to avoid recurrence. Because endoscopy
with cauterization has a lower likelihood of problems, it is a minimally
invasive method that may be recommended in some situations. All things
considered, a complete assessment is required for any patient with inexplicable
neck lumps, particularly on the left side, in order to guarantee a timely
diagnosis and suitable therapy.
REFERENCES
1. Daoud
FS. Branchial cyst: an often forgotten diagnosis. Asian J Surg 2005;28(3):174-178.
2. Tong
F, Liang Y, Khan MF, et al. A fatal case of severe neck abscess due to a third
branchial cleft fistula: morphologic and immunohistochemical analyses. Diagn
Pathol 2016;11(1):87.
3. Carta
F, Sionis S, Mascia L, Puxeddu R. Fourth branchial cleft anomaly: Management
strategy in acute presentation. Int J Pediatr Otorhinolaryngol
2014;78(9):1480-1484.
4. Aneeza
WH, Mazita A, Marina MB, Razif MY. Complete congenital third branchial fistula:
Does the theoretical course apply. Singap Med J 2010;51:e122-e125.
5. Watson
GJ, Nichani JR, Rothera MP, Bruce IA. Case series: Endoscopic management of
fourth branchial arch anomalies. Int J Pediatr Otorhinolaryngol
2013;77(5):766-769.
6. Kruijff
S, Sywak MS, Sidhu SB, et al. Thyroidal abscesses in third and fourth branchial
anomalies: Not only a paediatric diagnosis. ANZ J Surg 2015;85:578-581.
7. Verret
DJ, Mcclay J, Murray A, Biavati M, Brown O. Endoscopic cauterization of fourth
branchial cleft sinus tracts. Arch Otolaryngol Head Neck Surg
2004;130(4):465-468.
8. Huang
Y-C, Peng SSF, Hsu W-C. KTP laser assisted endoscopic tissue fibrin glue
biocauterization for congenital pyriform sinus fistula in children. Int J Pediatr
Otorhinolaryngol 2016;85:115-119.
9. Li
W, Xu H, Zhao L, Li X. Branchial anomalies in children: A report of 105
surgical cases. Int J Pediatr Otorhinolaryngol 2018;104:14-18.
10. Lachance
S, Chadha NK. Systematic review of endoscopic obliteration techniques for
managing congenital piriform fossa sinus tracts in children. Otolaryngology Head
Neck Surg 2016;154(2):241-246.
11. Ibrahim
M, Hammoud K, Maheshwari M, Pandya A. Congenital cystic lesions of the head and
neck. Neuroimaging Clin N Am 2011;21(3):621-639.
12. Hallak
B, Bouayed S, Leishman C, Sandu K. Residual fistula of fourth branchial arch
anomalies and recurrent left-side cervical abscess: clinical case and review of
the literature. Case Rep Otolaryngol 2014;2014:931279.
13. Nicoucar
K, Giger R, Pope HG Jr, Jaecklin T, Dulguerov P. Management of congenital
fourth branchial arch anomalies: a review and analysis of published cases. J
Pediatr Surg 2009;44(7):1432-1439.
14. Guldfred
LA, Philipsen BB, Siim C. Branchial cleft anomalies: Accuracy of pre-operative
diagnosis, clinical presentation and management. J Laryngol Otol
2012;126(6):598-604.
15. Neff
L, Kirse D, Pranikoff T. An unusual presentation of a fourth pharyngeal arch
(branchial cleft) sinus. J Pediatr Surg 2009;44(3):626-629.
16. Barberet
G, Diakhate I, Conessa C, Moriniere S. TDM et diagnostic des fistules de la
quatrieme poche branchiale chez l’adulte. J Radiol 2008;80:1676.
17. Givens
DJ, Buchmann LO, Park AH. A novel surgical management of hypopharyngeal
branchial anomalies. Int J Pediatr Otorhinolaryngol 2015;79(4):579-583.
18. Pereira
KD, Smith SL. Endoscopic chemical cautery of piriform sinus tracts: A safe new
technique. Int J Pediatr Otorhinolaryngol 2008;72(2):185-188.
19. Bajaj
Y, Ifeacho S, Tweedie D, et al. Branchial anomalies in children. Int J Pediatr
Otorhinolaryngol 2011;75(8):1020-1023.
20. Nicoucar
K, Giger R, Pope Jr GP, et al. Management of congenital fourth branchial arch
anomalies: A review and analysis of published cases. J Pediatr Surg
2009;44(7):1432-1439.
21. Sayadi
SJ, Gassab I, Dellai M, et al. [Laser coagulation in the endoscopic management
of fourth branchial pouch sinus]. Ann Otolaryngol Chir Cervicofac
2006;123(3):138-142.
22. Derks
LSM, Veenstra HJ, Oomen KPQ, Speleman L, Stegeman I. Surgery versus endoscopic
cauterization in patients with third or fourth branchial pouch sinuses: a
systematic review. Laryngoscope 2016;126(1):212-217.
23. Saadoun
A. Endoscopy for a fourth branchial cleft cyst. Am J Otolaryngol
2020;41:102623.
24. Kim
MG, Lee NH, Ban JH, Lee KC, Jin SM, Lee SH. Sclerotherapy of branchial cleft
cysts using OK-432. Otolaryngol Head Neck Surg 2009;141(3):329-334.