A Case of Gastrointestinal Bleeding Associated to Aortic Valve Stenosis
Keywords: aortic stenosis; anaemia, heyde’s syndrome; gastrointestinal bleeding
However, when the aortic valve was replaced, bleeding was alleviated in the majority of cases. Interestingly, replacing the aortic valve alleviated the bleeding in >90% of cases. In the early 2000s, the syndrome was further described to include severe aortic stenosis inducing an acquired von willebrand coagulopathy due to shear stress and gastrointestinal arteriovenous malformations (avms) causing moderate to significant bleeding3. An estimated 7-24% of patients with unknown origin of gastrointestinal bleeding were later found to have aortic stenosis4. Of patients found to have aortic stenosis with gastrointestinal bleeding, acquired von willebrand syndrome is seen in up to 67%5.
Severe aortic stenosis is defined as an aortic valve area ≤1.0 cm2, with an aortic velocity ≥4.0 m/s, and/or a mean transvalvular gradient ≥40 mmhg6. Generally a disease of the elderly, the prevalence of aortic stenosis varies from 0.2% at ages 50-59 years, to 1.3% at ages 60-69, 2.9% at ages 70-79, and 9.8% at ages 80-897. The classic clinical manifestations are heart failure, syncope, and angina. These manifestations are described in the context of cardiac symptoms. Here, we discuss a case of severe aortic stenosis with gastrointestinal bleeding.
1. Case presentation
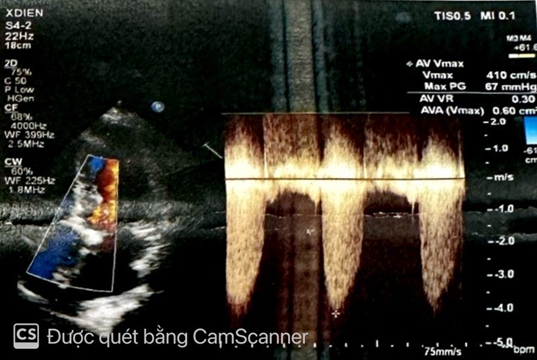
This case involves a 73-year-old woman who initially presented with weakness of lower extremities and dyspnea for two weeks duration. Her history diseases were hypertension, type 2 diabetes and lumbar spine osteoarthritis she had no significant cardiac family history with no history of sudden cardiac death. Physical examination was remarkable for a 3/6 crescendo systolic murmur heard best at the right upper sternal border. Electrocardiography showed sinus rhythm 95 bpm, left ventricular hypertrophy (figure 1). Chest xrays showed a large cardiac shadow (figure 2). Transthoracic echocardiography revealed a severe aortic valve stenosis, peak velocity of 4.10 m/s across the valve and peak gradient 67 mmhg (figure 3). The patient’s native aortic valve area was 0.6 cm2; moderate aortic valve regurgitation. Laboratory tests including routine full blood count showed moderate hypochromic microcytic anemia with hb: 7.4g/dl, renal and liver profiles were unremarkable. Abdominal ultrasound was normal.
figure 1. Electrocardiography showed sinus rhythm 95 bpm, left ventricular hypertrophy.
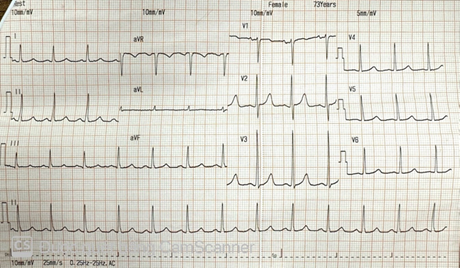
Figure 2. Chest xrays showed a large cardiac shadow.
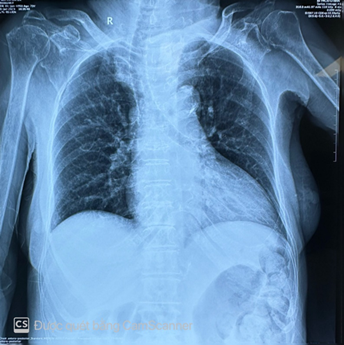
Figure 3. Continuous wave doppler echography revealed vmax 4.10
m/s, maximum pressure gradient 67 mmhg, ava 0.6 cm2.
She
electively underwent aortic valve replacement with a bioprosthesis. In the
perioperative period, the patient had no recurrent anemia. She was discharged
with no episode of recurrent gastrointestinal bleeding.
1. Discussion
Heyde's
syndrome is named after dr e c heyde who in 1958 described ten cases of aortic
stenosis and massive gastrointestinal bleeding for which he could discover no
cause2. The prevalence of the condition is unknown.
In one retrospective analysis, 2.6% of patients with aortic stenosis, compared
with 0.025% of a control group, had idiopathic gastrointestinal bleeding8. Subsequent reports have implicated gastrointestinal
angiodysplasia as a possible source of the bleeding but the precise relation
between aortic stenosis and angiodysplasia is unclear. A causal relation is
possible, but another possibility is that they coexist as age-related
phenomena.
The
blood vessel dilatation in gastrointestinal angiodysplasia is thought to arise
from long-term obstruction within the submucosal mesenteric venous system,
leading to loss of precapillary sphincters and formation of arteriovenous
communications. A possible mechanism for the bleeding in heyde's syndrome is an
acquired form of von willebrand's disease (type iia) due to the aortic
stenosis. High shear rates across the stenotic valve lead to increased
consumption of high-molecular-weight multimers of von willebrand factor (vwf).
The subsequent functional deficit of vwf predisposes to bleeding. In a recent
study, 21% of patients with severe aortic stenosis experienced skin or mucosal
bleeding. Most of the patients had vwf abnormalities, the severity of which related
to the degree of stenosis9. Gastrointestinal angiodysplasia may be
diagnosed by upper gastrointestinal endoscopy, enteroscopy, colonoscopy or
capsule endoscopy. The lesions are found most commonly in the small bowel.
For bleeding angiodysplasia, one treatment option is combined oestrogen and progesterone therapy, which can reduce transfusion requirements by up to half10. However, the possible benefits of hormone therapy should be set against cardiovascular risks. An alternative is to treat bleeding angiodysplasia at endoscopy with argon beam diathermy, but it is unknown whether this affects the natural history of the disease and risk of subsequent bleeding. Surgical options are bowel resection or aortic valve replacement. There have been several case reports of cessation of bleeding following aortic valve replacement11. In a retrospective study of 91 patients with aortic stenosis and unexplained gastrointestinal bleeding king et al. Found that bleeding ceased in 93% of patients treated by valve replacement compared with 5% of those managed by laparotomy with or without bowel resection12.
2. Conclusion
Doctor
need to be thoughtful and consider heyde syndrome in patients with severe
aortic stenosis and gastrointestinal bleeding secondary to angiodysplasia.
Doctors should also to be vigilant in patients with heyde syndrome presenting
with astrointestinal bleeding after undergoing aortic valve replacement, as
astrointestinal bleeding might take time to resolve completely in these
patients, assuming they had a successful aortic valve replacement.
3. Conflict of interest
None
declared.
References
1. Pate ge, mulligan a. An epidemiological
study of heyde's syndrome: an association between aortic stenosis and
gastrointestinal bleeding. J heart val dis 2004;13(5):713-716.
2.
Hyde j. Gastrointestinal bleeding in
aortic stenosis. Ejnejm 1958;259:196.
3.
Blackshear
jljcigm. Heyde syndrome: aortic stenosis and beyond. Clin geriatr med
2019;35(3):369-379.
4. Shoenfeld
y, eldar m, bedazovsky b, levy mj, pinkhas j. Aortic stenosis associated with
gastrointestinal bleeding. A survey of 612 patients. Am heart j
1980;100(2):179-182.
6.
Walker bl, williman mc, patel m, houle mc,
thomas jm. A case of heyde’s syndrome with subvalvular aortic stenosis. Cureus
2022;14(11):e31723.
7.
Gry
wisthus e, henrik s, geir h, per l, knut r. The evolving epidemiology of
valvular aortic stenosis. The tromsø study. Heart 2013;99(6):396-400.
8.
Cody mc, o'donovan tpb, hughes rw.
Idiopathic gastrointestinal bleeding and aortic stenosis. Am j digest dis
1974;19:393-398.
9.
Vincentelli a, susen s, le tourneau t, et
al. Acquired von willebrand syndrome in aortic stenosis. New eng j med
2003;349(4):343-349.
11. Anderson
r, mcgrath k, street a. Reversal of aortic stenosis, bleeding gastrointestinal
angiodysplasia, and von willebrand syndrome by aortic valve replacement. Case
rep 1996;347(9002):689-690.
12. King rm, pluth jr, giuliani er. The association of unexplained gastrointestinal bleeding with calcific aortic stenosis. Ann thorac surg 1987;44(5):514-516.