A Case Report of Strangulated Small Bowel Spigelian Hernia and Literature Review
Abstract
Spigelian hernia is considered one of
the rarest types of hernias, accounting for only 2% of all abdominal hernias. It is a type of ventral hernia,
defined as a defect in the abdominal wall lateral to the rectus abdominus muscle. In the current case report, we present a case of an elderly man who developed a strangulated Spigelian hernia. He was taken to an emergency surgery, where he had a strangulated
ischemic small bowel segment. It ended up by resection, anastomosis, and repair
of the hernia defect. He had an uneventful post-operative recovery and was
discharged in good condition.
Keywords: Intestinal obstruction; Spigelian hernia; Open
hernia repair; Laparoscopic repair
Introduction
The incidence of Spigelian hernia is 0.2-2%. It is considered one of the rarest types of abdominal wall defects. Spigelian hernia is a ventral hernia, raised from Spigelian fascia. It
lies medial to the semilunar line and lateral to the outer edge of the rectus
abdominis muscle1,2. It is more predominant among females. However, risk factors are similar to those related to other
abdominal wall defects which include old age, obesity,
multiparous, and abdominal trauma2,3.
Patients usually present to the ER with vague clinical symptoms and signs, the
diagnosis are considered a challenge. At the first visit, it is usually complicated with incarceration. The clinical diagnosis can be confirmed by radiological
examinations, such as ultrasound or CT scans. The need for surgical management
is crucial once the diagnosis has been
established, due to the high risk of strangulation which can reach up to 24%1,4. The
operative approach can either be done with open surgical repair or laparoscopic
such as TEP, TAPP, or IPOM1.
Case presentation
96-year-old male patient presents with a history of reducible
right direct inguinal hernia for a long time. He suddenly developed a small
tender swelling at the right iliac fossa lateral to the rectus muscle, not
reducible for one day. It was
associated with constipation and repetitive vomiting. Clinically, the patient was in pain
with a reducible right inguinal hernia but irreducible right lateral tender swelling, about 2*3
cm with negative cough impulse.
Impression was incarcerated ventral hernia. The patient was taken to the operating theatre and an incision made over the swelling
showed intact external oblique fascia with a herniated bowel underneath the
fascia (Figure 1). The bowel was ischemic, and consequently, resection and
anastomosis were performed without
mesh. The patient stayed a few
days in the hospital and then discharged after fully recovered.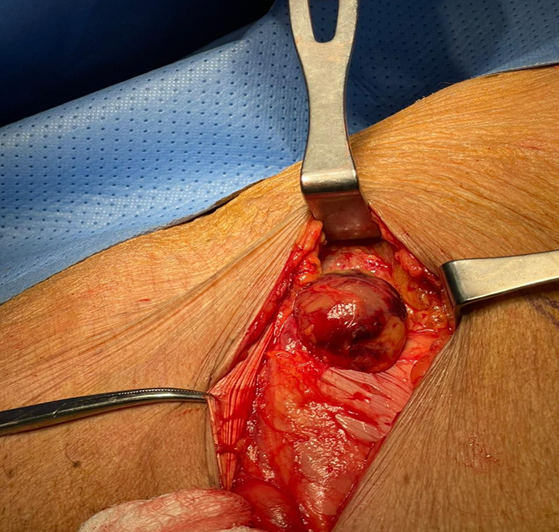
Figure 1: Implies right spigelian
incarcerated hernia with ischemic bowel content.
Discussion
Spigelian hernia needs high index of
suspicion due to its rarity and the nature of ambiguous clinical presentation
as the external oblique fascia is preserved which
gives its obscured examination to determine the hernia site2,3. Adrian
van den Spiegel was the first surgeon to describe it (1578-1625). It protrudes through a congenital or
acquired defect in the Spigelian aponeurosis. It consists of transversus
abdominis and internal oblique muscle fusion] between the semilunar line and
the rectus muscle1,5. 90% of the
cases are located infra
umbilically at the Spiegel line3. The
content might include preperitoneal fat, peritoneal sac, colon, appendix,
ovary, testicle, and endometrial tissue, while the most expected organ is the
small bowel1,3. The manifestation of a
Spigelian hernia includes chronic intermittent abdominal pain, bulge at the
abdominal wall, and sometimes symptoms resemble small or large bowel
obstruction1,5 pain percentage varies between 31% and 86%1. As the neck
of a Spigelian hernia is usually narrow, it poses a high incarceration risk and it mandates prompt surgical repair6. Diagnosis can be challenging by the physical
examination solely. Therefore, it is advisable to proceed with either
ultrasound or CT scan of the abdomen and
pelvis. They can identify the location of the defect, assess the
contents of the sac, detect any bowel obstruction or ischemia, and evaluate the
layers of the abdominal wall3,5.
The treatment of spigelian hernia is
surgical, either open or laparoscopic repair. The open technique is defined as a
transverse incision with primary repair of the defect. Laparoscopic repair has
different approaches including
transabdominal pre-peritoneal (TAPP), total extra-peritoneal (TEP), and
intraperitoneal on-lay mesh (IPOM) repair. IPOM is considered the most popular
amongst all types of laparoscopic approaches due to its simplicity and shorter
operation time1,5. In emergencies,
open repair with or without mesh is more practical than the laparoscopic
approach, particularly in cases of strangulation or incarceration where there
is a risk of bowel ischemia. However, the laparoscopic approach offers
advantages such as shorter hospital stays and smaller incisions that results in
less postoperative pain. While mesh has an advantage
to decrease recurrence rate, it was not used in our case due to concerns
about bacterial translocation in the presence of gangrenous bowel5. The long-term
recurrence rate was reported to be lower with mesh contrary to simple suture
closure2.
In a single center experience that
performed a retrospective study by6
reported 8 spigelian hernia cases with right sided in seven cases, and left
side in one case. In addition, two of their cases accompanied with inguinal
hernia and one other had an umbilical hernia3.
Moreover7,8, highlighted that
Spigelian hernias are often underdiagnosed and are more common than previously
thought. These hernias can manifest in three clinical stages. Stage 1 hernias,
which lack peritoneal sacs, are typically found in younger patients. On the
other hand, Stages 2 and 3 hernias, which involve peritoneal sacs, tend to
occur in older individuals and may present as emergencies8.
Spigelian hernias can be evaluated
using various radiological methods. A study conducted by D Light et al from
1998 to 2010, revealed that CT scan exhibited a sensitivity and positive
predictive value (PPV) of 100%, while ultrasound sensitivity was 90% and a PPV
of 100%. In contrast, comparing to clinical assessment, the sensitivity was
100% but the PPV was only 36%8.
There was a study compared open
versus laparoscopic repair in elective bases, reported that the laparoscopic
hernia repair superior in terms of morbidity and hospital stay9. T Mittal et al have shown a comparison between
different laparoscopic approaches to repair Spigelian hernia, hernia repairs were done either by IPOM, TAPP, or
TEP. Despite different laparoscopic methods, no recurrence or morbidly
were observed for up to 10 years of follow-up respectively10,11.
Conclusion
In conclusion, the detection and
diagnosis of Spigelian hernia represent challenges due to their rarity and
non-specific symptoms. Surgical repair, whether open or laparoscopic, remains
the gold standard for treatment. The laparoscopic approach offers benefits such
as reduced hospital stays and smaller incisions, but the choice of technique
should be tailored to the individual patient. The common site of the hernia is
the right side and oftenly associated with another defect. However, the
long-term outcomes of laparoscopic and robotic techniques remain unclear in the
current literature, highlighting the need for further research in this area to
enhance our understanding and optimize patient care.
References
1. Goswami AG, Huda F, Singh SK, Kumar N, Basu S. Spigelian
Hernia: Clinical features and management. Hernia
Surgery 2022.
2. Qin NGZ, Low W, Subramanian P, Joel S.
Strangulated small
bowel in a spigelian hernia and a review of the literature. Ann Emerg Surg 2017;2(2):1011.
3. Larson DW, Farlev DR. Spigelian Hernias: Repair and outcome for
81 patients. World J Surg 2002;26(10):1277-1281.
4. Takayama Y, Okada S, Nakatani K,
Matsumoto R, Suganuma T, Rikiyama T. The advantage of laparoscopic surgery in the treatment of Spigelian hernia: A report of two
cases. Int J Sur Case Rep 2021;82:105903.
5. Jamshidian M, Stanek S, Sferra J, Jamil T. Robotic repair of
symptomatic Spigelian hernias: A series of three cases and surgical technique
review. J Robotic Surgery 2018;12(3):557-560.
6. Ali CM, Karim N, Asma C, Ben KM, Moez
B. Spigelian hernia: A single-center experience in an
uncommon hernia. Int
J Abdominal Wall Hernia Sur 2019;2(2):59-62.
7. Sundar G, Shetty SK. A rare case
report of strangulated spigelian hernia mimicking an abdominal mass. Indian J Case Rep 2022;8(3):69-71.
8. Webber V, Low C, Skipworth RJE, Kumar S, de Beaux AC, Tulloh
B. Contemporary thoughts on the management of Spigelian hernia. Hernia 2017;21(3):355-361.
9. Light D, Chattopadhyay D, Bawa S. Radiological
and clinical examination in the diagnosis of Spigelian hernias." Annals of
the Royal College of Surgeons of England 2013;95(2):98-100.
10. Moreno-Egea A, Carrasco L, Girela E,
Martin J-G, Aguayo JL, Canteras M. Open vs laparoscopic repair of spigelian
hernia: A prospective randomized trial. Arch sur 137,11 (2002):1266-1268.
11. Mittal T, Kumar V, Khullar et al. Diagnosis
and management of Spigelian hernia: A review of literature and our experience.
Jo minimal access surgery 2008;4(4):95-98.