A Rare Case of Krukenberg Tumor in a Young Female Initially Misdiagnosed as Ovarian Tuberculosis
Abstract
Krukenberg tumour is a metastatic ovarian tumour made up of mucin-rich
signet-ring cells. The stomach is the most typical initial location for this
tumour. The lymphatic system is most likely how these tumours spread. We
describe a remarkably unusual case of a 28-year-old woman who presented with a
krukenberg tumour with an unknown primary focus. This case is an exceptional
incidence of a young person developing metastatic carcinoma with an unknown
primary focus presenting as a krukenberg tumour. The patient's initial
complaints were abdominal pain and nausea. The initial workup of the patient
revealed bilateral ovarian tumours, which were incorrectly treated as ovarian
tuberculosis. A ct scan and further studies revealed deposits in the peritoneum
and omentum, which were suggestive of metastatic illness. Laparotomy was
performed and biopsies from the ovarian tumors were taken to investigate other
diagnoses. Signet-ring cells were discovered through immunohistochemical and
histopathological analyses, supporting the diagnosis of a metastatic krukenberg
tumour with an unknown primary focus.
Keywords: krukenberg tumour; peritoneum;
omentum
Introduction
Adult tumours that spread to the ovaries
commonly do so; in fact, 5-30% of ovarian cancer cases are metastatic diseases.1
adenocarcinoma with pleomorphic mucin-filled signet-ring cells, initially
described by krukenberg in 1896, accounts for approximately 5% of all
carcinomas that have spread to the ovaries.2 this
tumour is also known as the krukenberg tumour. The stomach (which accounts for
70% of cases) is the most typical location of the primary tumour in this
patient group, followed by the large bowel, appendix, and occasionally several
other sites.1,3 however, the primary tumour can go undetected
in 25% of the cases because it is very small. The involvement of the ovary,
which is typically bilateral and can take on enormous proportions, is assumed
to be the result of the selective retrograde lymphatic spread of the initial
tumour along the stomach-ovarian axis.4 with a
median life span of 14 months, individuals with krukenberg tumours typically
die, as there is currently no viable treatment available.5
due to their vague clinical manifestations and similarities to benign
illnesses, such as ovarian tb, krukenberg tumours are renowned for being
diagnostic dilemmas. To highlight the need for accurate differential diagnosis
in treating unusual neoplastic disorders, we provide an example of a
28-year-old female patient with a krukenberg tumour who was initially
misdiagnosed as having ovarian tuberculosis.
Case presentation
A 28-year-old female patient presented with
abdominal pain, bloating, decreased appetite and irregular menstrual cycles to
a physician who suspected her to be a case of ovarian tuberculosis (tb) based
on her symptoms and computed tomography (ct) findings which initially showed
suspicion of tuberculosis and put her on anti-tuberculous therapy (att). Three
months later, she presented to our emergency department with worsening symptoms
and ascites. Based on her ct findings, we suspected ovarian tb but her
unresponsiveness to att forced us to consider an alternate diagnosis. To be
safe, we started a workup to rule out any malignancy. The patient presented
with complaints including nausea, abdominal pain, and decreased appetite. The
patient experienced severe discomfort due to abdominal pain. On examination,
she was cachexic, her abdomen was mildly tender, and there were ascites with
dullness to percussion. The rest of the examinations were unremarkable. Except
for lower blood pressure, the other vital signs were stable. Large
heterogeneous cystic mass lesions with irregular margins and ascites were
observed on abdominal ultrasonography (us). Computed tomography (ct) showed a
large well-defined heterogeneous cystic mass lesion with irregular lobulated
margins, measuring approximately 10 x 11 cm, which is noted in the left adnexa.
The lesion appears to arise from the left ovary. It had a small solid
peripheral enhancing component and a large internal non-enhancing necrotic
area. It had thin enhancing walls with few septations. The lesions have a
distinct interface with the surrounding structures and do not invade the gut
loops or pelvic walls. Posteriorly, the lesion did not extend to the pelvic
sidewall or rectum. Superiorly, the lesion extended into the lower abdomen with
the displacement of the bowel in the region. There was no evidence of
calcification or haemorrhage within or adjacent to the lesion. Another large
heterogeneous enhancing lesion was seen in the right adnexa measuring 5.3 x 3
cm. The right ovary was visualized separately from the lesion shown in (figure 1).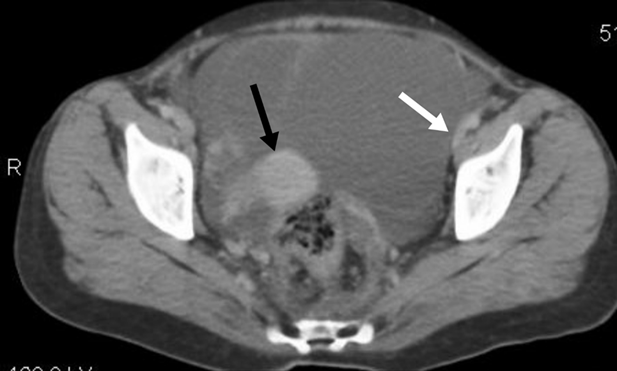
Figure 1. Black arrow shows right ovarian
lesion. White arrow shows peritoneal involvement.
The uterus was
normal in both size and shape. Focal lesions were not observed. Multiple
enlarged, rounded, and enhancing lymph nodes are seen in the pelvis. Gross
abdominopelvic ascites were observed. No scalloping of the abdominal viscera
was observed, and multiple large soft tissue density-enhancing deposits of
variable sizes were seen in the omentum, predominantly on the left side of the
abdomen measuring 2.8 x 1.5 cm as shown in (figure 2).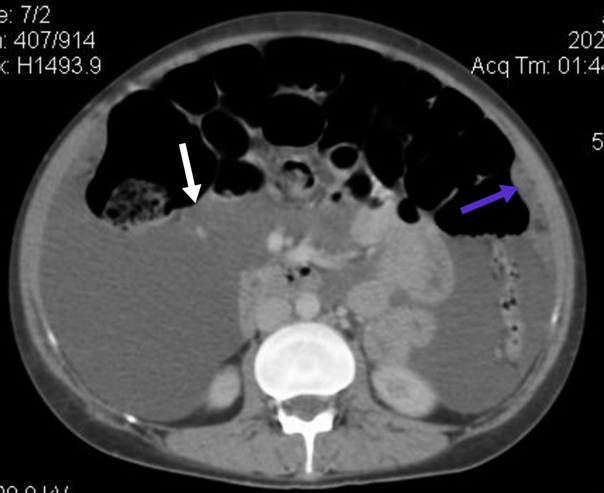
figure 2. White arrow showing ascities. Blue arrow showing omental
deposits.
All of these
findings were suggestive of ovarian malignancy with metastasis. Except for
slightly high serum levels of ca 19-9 equals 41.9 u/ml (normal values 0 - 37),
ca 125 equals 73.26 u/ml (normal values 0 - 37), and chromogranin a 37.0 u/l
(normal values 2 - 18), the findings of the laboratory work-up were within
normal ranges. The impression given by the imaging of a large tumour
potentially harming the ovarian tissue was confirmed by laparotomy. Due to the
lack of adhesions between the masses and the nearby organs and tissues, the
excision of both masses together with bilateral salpingectomy was completed
after obtaining informed consent on the basis that ovarian function had been
lost. Exploration of the abdominal cavity revealed tumour deposits and ascites
in multiple areas. Masses and metastatic lesions were removed and sent for
histopathological analysis. Histopathology gave the following reports on gross
examination of a skin-covered tissue piece separately present in containers
along with bilateral fallopian tubes. The uterus measured 40 mm × 33 mm × 24
mm. On serial slicing, the endometrial cavity measured 20 mm × 2 mm. The
maximum thickness of the endometrium was 1 mm, and that of the myometrium was
14 mm. A fibroid (separately present in the container) measured 20 mm × 19 mm ×
15 mm. Serial slicing revealed a tan-white whorled cut surface. The
skin-covered tissue piece measured 21 mm × 19 mm. The skin was grossly
unremarkable. The soft tissue fragments measured 135 × 65 × 30 mm. The first
fallopian tube measured 45 mm × 9 mm. The second fallopian tube measured 51 mm
× 9 mm. The cut surfaces of both fallopian tubes were unremarkable. Microscopic
examination revealed a malignant tumour made up of sheets of signet-ringed
cells diffusely invading multiple tissue fragments. Immunohistochemical
findings are shown in (table 1).
table
1. Immuno/histochemical stain(s)
|
Stain (s) |
Results |
|
Ck7 |
Patchy positive |
|
Ck20 |
Positive |
|
Cdx2 |
Positive |
|
Mucin |
Positive |
|
Pax8 |
Negative |
Ck - cytokeratin; cdx -
caudal-related homeobox transcription factor; pax - paired-box gene
The bilateral fallopian tubes were tumour-free.
Skin tissue showed fibrosis. Endometrial leiomyoma is a signet-ring cell
adenocarcinoma. A metastatic diagnosis of signet ring cell cancer was made. A
suspected primary tumour was investigated after an uneventful postoperative
course, which included breast and thyroid ultrasound, oesophagal gastroduodenal
and ileum colorectal endoscopy and hysteroscopy; however, no primary focus
could be found despite immunohistochemical staining pointing towards colon
cancer. Following the laparotomy, her clinical condition continued to
deteriorate, and she was moved to a high-density unit (hdu) and a subsequent
intensive care unit (icu). Before starting chemotherapy and discussing her with
the oncologist, she deteriorated and died a month after the exploratory laparotomy.
Discussion
Conclusion
Conflicts of interest
This study does not have any conflict of interest.
References
1. Young rh, scully re. Metastatic tumors of the ovary. Inblaustein’s pathology of the female genital tract. New york, ny: springer new york 1987;742-768.
2. Krukenberg fe. Fibrosarcoma ovarii microcellular (carcinomatdes). Arch gynecol 1896;50:287-321.
3. prat j. Ovarian carcinomas, including secondary tumors: diagnostically challenging areas. Mod pathol 2005;18:99-111.
4. young rh. From krukenberg to today: the ever present problems posed by metastatic tumors in the ovary. Part ii. Adv anat pathol 2007;14(3):149-177.
5. al-agha om, nicastri ad. An in-depth look at krukenberg tumor: an overview. Arch pathol lab med 2006;130(11):1725-1730.
6. kiyokawa t, young rh, scully re. Krukenberg tumors of the ovary: a clinicopathologic analysis of 120 cases with emphasis on their variable pathologic manifestations. Am j surg pathol 2006;30(3):277-299.
7. berens jj. Krukenberg umors of the ovary. American j surg 1951;81(5):484-491.
8. khurana p, sachdev r, uppal s, bisaria d. Krukenberg tumor in a 13-year-old girl: a rare occurrence. Indian j pathol microbiol 2010;53(4):874-875.
9. kim hk, heo ds, bang yj, kim nk. Prognostic factors of krukenberg's tumor. Gynecol oncol 2001;82(1):105-109.
10. kim a, ueda y, naka t, enomoto t. Therapeutic strategies in epithelial ovarian cancer. J exp clin cancer res 2012;31:1-8.
11. gupta p, snebold ma, o'donnelly s. Krukenberg's tumor in the young population. J am osteopath assoc 1989;89(4):500-502.