A Rare Case of Merkel Cell Carcinoma of the Eyelid
Keywords: merkel cell carcinoma; eyelid; surgery
Introduction
Merkel cells were first identified by friedrich merkel in
18751 and are in the basal layer
of the epidermis, near the dermo-epidermal junction and in certain mucosal
tissues, excluding the conjunctiva. Initially believed to function as
mechanoreceptors (tactile sensory cells), these neuroendocrine cells are now
thought to originate from the neuroectoderm and migrate to the skin alongside
peripheral nerves. In 1978, tang and toker described the malignancy of these
cells, which became known as merkel cell carcinoma2.
This cancer typically begins in the dermis, sparing the epidermal layer above
it. Despite its neuroendocrine nature, merkel cell carcinoma is not associated
with hormonal syndromes3.
Case report
This study reports the case of an 87-year-old woman
admitted to the ent and maxillo facial department of spaziani hospital,
frosinone, italy unit with a violaceous mass on her upper eyelid (figure 1). During her hospitalization, an excisional biopsy
was performed, ensuring clear margins. Local hemostasis was performed with
absorbable hemostat of oxidized regenerated cellulose with neutral ph (oxitamp
powder®, assut europe) followed by a primary intention closure of the wound
with non-absorbable suture (assuplus®, assut europe). The tumor,
described as a nodular, exophytic, solid and reddish mass, showed no signs of
lymph node involvement or distant metastasis during the initial evaluation.
Based on the american joint committee on cancer (ajcc) classification system,
the tumor was staged as t2n0m0 after the oncological surgery.

Figure 1: a clinical image shows a patient with merkel cell carcinoma affecting the upper right eyelid. The tumor presents as a nodular, exophytic, solid and reddish lesion, causing mechanical ptosis due to its size and location.
The diagnosis was confirmed through
histopathological evaluation, supported by immunohistochemical testing:
The histological analysis of a 2.5 cm skin biopsy, stained with hematoxylin and eosin, revealed an ulcerated epidermis. The superficial and deep dermis were extensively infiltrated by poorly differentiated neoplastic cells arranged in a solid growth pattern.
Cytological evaluation showed these cells had scant cytoplasm and round, well-defined, polymorphic nuclei displaying a characteristic "salt-and-pepper" chromatin pattern, with inconspicuous nucleoli. At 40x magnification, a mitotic index of seven mitotic figures per eight high-power fields was observed, along with scarce apoptotic cells. The tumor stroma contained minimal connective tissue strands and few vessels, some of which exhibited neoplastic embolization. No areas of necrosis were identified.
Immunohistochemical staining demonstrated positive
expression for ck20, chromogranin and synaptophysin, while markers such as
cdx2, s100 and pan-leu were negative. Based on the morphological and
immunohistochemical findings, the diagnosis was consistent with merkel cell
carcinoma of the skin. Notably, there was no involvement of the epidermis (figure 2).
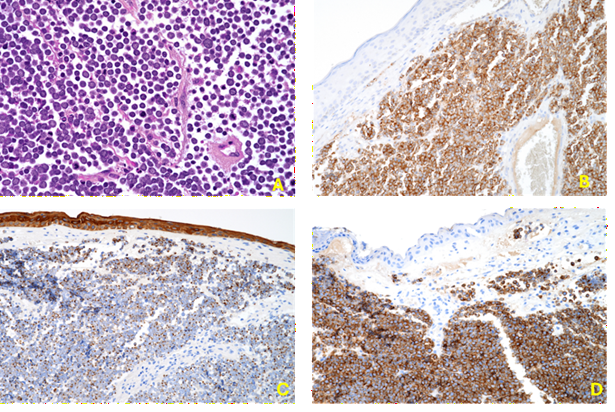
Figure 2: a: hematoxylin-eosin (h&e) staining (40x); b: pan cytokeratin immunostaining (20x); c: synaptophysin immunostaining (20x); d: chromogranin immunostaining (20x).
Despite the success of the procedure, further follow-up could not be carried out, as the patient unfortunately passed away due to cardiac complications unrelated to the cancer.
Discussion
Merkel cell carcinoma is a rare and aggressive form of skin
cancer, with a mortality rate surpassing that of melanoma (46% vs. 15% over
five years). In this case report, the patient's death was not directly linked
to the carcinoma. Studies from the u.s. indicate an increase in incidence from
0.15 to 0.6 per 100,000 individuals between 1986 and 2006. This cancer
primarily affects those over 65 years, particularly caucasians and
immunocompromised individuals, such as those with chronic lymphocytic leukemia,
hiv or organ transplants3,4.
Gender differences are unclear, though some studies suggest a higher prevalence among women (2:1 ratio). About 35-47% of cases occur in sun-exposed areas like the head and neck, especially the cheeks and eyelids, with 5-10% affecting the eyelids. The remainder are found on the limbs (40%) and torso or genitals (10%). In rare cases, the carcinoma may appear simultaneously in multiple locations, a condition known as merkeliomatosis.
It has been observed that merkel cell carcinoma tends to occur more frequently in the upper eyelid compared to the lower eyelid, with a distribution of 71% versus 21%. In our case report, the tumor affected the upper eyelid, consistent with this trend. This predilection for the upper eyelid could be related to greater sun exposure or anatomical factors that make this area more susceptible to tumor development. The mass was nodular and exophytic, leading to mechanical ptosis, further emphasizing the tumor's significant impact on the upper eyelid.
It has been observed5 that sequences within the genome of merkel cell carcinoma cells are compatible with a newly identified polyomavirus. This virus may infect carcinoma cells, integrating its genetic material and potentially leading to long-term cell cycle disruption. Although the exact mechanism remains unclear, research has shown that approximately 85% of merkel cell carcinoma cases contain cells infected with this polyomavirus, strongly supporting the hypothesis that the virus plays a significant role in the development of the carcinoma.
The macroscopic differential diagnosis for merkel cell carcinoma includes conditions such as chalazia, basal cell carcinoma, nodular angiosarcoma and metastatic tumors. These conditions can mimic the appearance of merkel cell carcinoma, making it essential to consider a broad range of possibilities during diagnosis to avoid delays in appropriate treatment.
The national comprehensive cancer network (nccn) in the
united states has established guidelines for the diagnostic evaluation of
merkel cell carcinoma (mcc), following a structured approach based on clinical
presentation, initial work-up, diagnosis and further evaluation (figure 3)6,7. Once mcc is confirmed through clinical
and histopathological findings, appropriate staging should be conducted. For
patients with palpable lymph nodes, fine-needle aspiration or core biopsy is
recommended. In cases with clinically negative lymph nodes, sentinel lymph node
biopsy (slnb) is considered the most accurate method for assessing regional
lymph node involvement. Slnb is advised as approximately 25% to 30% of patients
with clinically negative nodes are found to have pathological nodal involvement8.

Figure 3: management of merkel cell carcinoma according to stage. Sr: 5 years survival rate
Conclusion
In conclusion, early detection and extensive tumor excision
with intraoperative margin evaluation, whether through conventional surgery or
mohs micrographic surgery, paired with appropriate eyelid reconstruction, are
key to improving survival outcomes in elderly patients with merkel cell
carcinoma of the eyelid. Current evidence supports incorporating sentinel lymph
node biopsy during the initial procedure, along with adjuvant radiotherapy.
This combined approach not only reduces the risk of local recurrence but also
enhances survival by addressing both the primary tumor and any early metastatic
spread.
Conflicts
of interest
The
authors declare no conflict of interest.
References
1. Halata
z, grim m, bauman ki. Friedrich
sigmund merkel and his “merkel cell,” morphology, development and physiology:
review and new results. Anat rec a discov mol cell evol biol 2003;271:225-239.
2. Tang ck, toker c. Trabecular carcinoma of the skin: an
ultrastructural study. Cancer 1978;42:2311-2321.
3. Senchenkov a, moran sl. Merkel cell carcinoma: diagnosis,
management and outcomes. Plast reconstr surg 2013;131(5):771e-778e.
4. Albores-saavedra j, batich k, chable-montero f, sagy n,
schwartz am, henson de. Merkel cell carcinoma demographics, morphology and
survival based on 3870 cases: a population-based study. J cutan pathol 2010;
37:20-27.
5. Feng h, shuda m, chang y, moore ps. Clonal integration of a
polyomavirus in human merkel cell carcinoma. Science 2008;319:1096-1100.
6. Lemos bd, storer be, iyer jg, et al. Pathologic nodal
evaluation improves prognostic accuracy in merkel cell carcinoma: analysis of
5823 cases as the basis of the first consensus staging system. J am acad
dermatol 2010; 63:751-761.
7. Edge sb, byrd dr, compton cc, et al. Ajcc cancer staging
manual 2010;1.
8. Gupta sg, wang lc, peñas pf, gellenthin m, lee sj, nghiem p.
Sentinel lymph node biopsy for evaluation and treatment of patients with merkel
cell carcinoma: the dana-farber experience and meta-analysis of the literature.
Arch dermatol 2006;142:685-690.