A Rare Case of Primary Thyroid Lymphoma: Case Report and Literature Review
Abstract
Primary lymphomas of the thyroid gland are rare and
very uncommon, representing less than 5% of thyroid neoplasia and occur more
frequently in women than in men, it develops in most cases on a pre-existing
thyroid condition, in particular Hashimoto's thyroiditis.
It's an aggressive pathology, presenting as a painful
goiter with rapid onset and compressive signs. To better understand this
entity, we report the case of a 65-year-old patient, with no history of chronic
thyroiditis, admitted for a rapidly progressive, hard and fixed anterior
cervical mass, accompanied by signs of compression. Initially suspected as an
anaplastic carcinoma, the patient was scheduled for total thyroidectomy.
However, during surgery, invasion of adjacent thyroid tissue was noted, justifying
partial tumor reduction. Definitive pathological examination, supported by
immunohistochemistry, confirmed the diagnosis of thyroid lymphoma.
Treatment consisted of exclusive chemotherapy and the
clinical evolution was very favorable.
Keywords: Primary thyroid lymphoma; Chemotherapy; Immunohistochemistry;
Chronic thyroiditis
Introduction
Primary lymphomas of the thyroid gland are unusual and
very uncommon. They account for around 5% of thyroid tumors and 2% of
extra-nodal lymphomas1-3.
Its annual incidence is estimated at 2 per 1 million
inhabitants, most often affecting patients with a median age of 60, with a
predominance of females, the sex ratio being 3:14.
Patients with Hashimoto's thyroiditis have an
increased risk of developing this disease compared to patients without
thyroiditis, with a relative risk of 675.
There are 70% cases of diffuse large B-cell lymphoma,
followed by 10 to 23% of MALT (mucosa-associated lymphoid tissue) lymphoma7. The most typical form is a rapidly
growing cervical mass, often adherent to adjacent tissues, which becomes
compressive in about a third of cases6.
The diagnosis of certainty is based on histology, and
the therapeutic course of action depends essentially on the histological type
and stage of the tumor.
Surgical indications, previously predominant, have
been restricted with the advent of new chemotherapy protocols which have become
the standard treatment for thyroid lymphoma.
Observation
Its
A 65-years-old female patient, with no significant medical history or known
thyroid issues, who was referred to us for a lower anterior cervical swelling
rapidly increasing in volume evolving since 4 months, associated to a dyspnea
to the effort and dysphagia to solids, without dysphonia or any other
associated signs, all evolving in a context of alteration of the general state.
The
physical examination revealed a large goiter, painless, with a non-palpable
lower edge, hard and fixed to the deep plane, with an irregular surface, but
without any inflammatory-looking or notion of lymphadenopathy.
The
Cervical ultrasound performed showed a heterogeneous goiter depending on the
right lobe and isthmus without any visible nodule.
A
cervicothoracic CT scan was ordered (because of the strong suspicion of
anaplastic carcinoma), which showed a general increase in the size of the
thyroid with multiple nodules, especially in the right lobe slightly plunging
towards the upper mediastinum and pushing the adjacent tissue structures,
moreover, the examination did not reveal any pulmonary involvement or
cervico-mediastinal lymphadenopathy (Figure
1).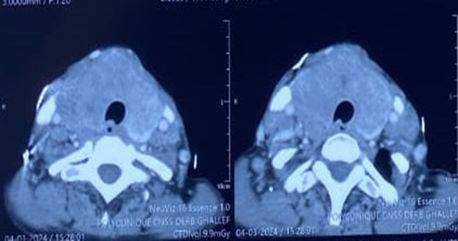
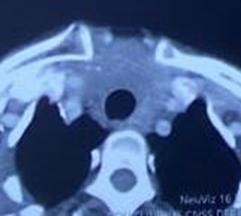
Figure1: Axial
CT images showing: an enlarged thyroid gland extending beyond the
cervicothoracic contour Biological
tests were normal, in particular the TSH us level, which was 5 mui/l.
Biological
tests were normal, in particular the TSH us level, which was 5 mui/l.
Intraoperatively,
the thyroid was clearly suspicious of malignancy, with massive invasion of the
trachea and larynx. The 2 recurrent nerves were engulfed by the tumour, and
surgery was stopped after removing a part of the right lobe of the thyroid (Figures 2,3).
Figure
2: Image the thyroid gland intraoperatively (after tumor
reduction).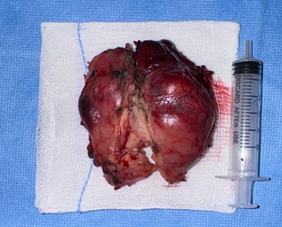
Figure 3:
Operative piece of the thyroid gland.
Postoperatively,
the patient presented respiratory distress for which she benefited from a
tracheotomy on day 4 (Figure 4). 
Figure 4:
Image of the neck after tracheotomy.
The
definitive histopathological examination showed the presence of a diffuse
cellular infiltrate with round cells (lymphoma?) And the complementary
immunohistochemical study revealed a diffuse large cell B lymphoma. Two months
after surgery, the patient was referred to the clinical hematology department
with the diagnosis of HL where she benefited from treatment with chemotherapy
according to the CHOP protocol (Cyclophosphamide, Doxorubicin, Vincristine and
Prednisone). The clinical evolution was favorable from the first course of
chemotherapy, with obvious regression of the thyroid tumor volume.
Discussion
Thyroid lymphomas are extremely rare, whether primary
or secondary8.
They represent approximately 5% of all thyroid cancers9.
Their incidence is estimated at 1.1 to 2.06 per
million inhabitants per year, this incidence has seen a clear increase in
recent years10,11. However, the
incidence of this disease is not yet documented in Morocco.
Patients are often female and generally consult during
the sixth or seventh decade, presenting compressive symptoms such as dyspnea,
and dysphagia associated with general symptoms such as weight loss, sweating or
fever in 10% of cases12.
Apart from dysphonia, all these symptoms were reported
by our patient during his first consultation. The consultation time can vary
from a few days to 36 months13.
This disease is closely associated with Hashimoto's
thyroiditis5, this association
was observed in 25 to 100% of cases according to published studies14-16.
Different theories have been put forward to explain
the HT/PTL association, it has been proposed that chronic and continuous
stimulation of lymphocytes by antigens could lead to lymphocyte proliferation
whose mutations lead to malignant differentiation causing lymphoma in the
thyroid gland. Which is normally a gland devoid of lymphoid tissue17,18.
The clinical picture is characterized by a rapidly
growing thyroid tumor, leading to compressive signs in 20 to 25% of cases19.
This goiter can sometimes be adherent to surrounding
tissues, and the presence of pain would strongly support the diagnosis;
satellite cervical lymphadenopathy is observed in 20% of cases20,21.
Biological hypothyroidism is present in almost 40% of
cases, although its clinical expression is rare20.
The diagnosis is confirmed in 61% of cases by fine
aspiration22,23, it helps to
differentiate lymphoid proliferation from epithelial tumor6. Ultrasound-guided biopsy has also
demonstrated higher diagnostic accuracy because it can obtain more tissue than
fine-needle aspiration cytology and thus distinguish between Hashimoto's
thyroiditis, thyroid lymphoma and anaplastic carcinoma24.
Historically, surgery and radiation therapy were the
standard treatments for primary thyroid lymphoma. Before retrospective studies
demonstrated that LT is sensitive to chemotherapy and radiotherapy.
The interrogation, the clinical examination, the
biological and radiological explorations in our patient all pointed towards a
strong suspicion of anaplastic carcinoma so the cytopuncture was not carried
out in our patient and the discovery of
tumor invasion of adjacent structures was only noted intraoperatively,
necessitating interruption of the surgical procedure after achieving tumor
reduction while preserving essential structures such as recurrent nerves, while
awaiting the results of the definitive histology.
Conclusion
Thyroid lymphoma is a rare disease often neglected and
underdiagnosed, requiring increased vigilance when observing any goiter or
thyroid nodule rapidly increasing in size with signs of compression. This will
enable early suspicion of the diagnosis and potentially avoid excessive surgery
for the patient.
References
1. Andeh MV, Memsic L, Silberman A. Anaplastic carcinoma,
lymphoma, unusual malignancies and chemotherapy for Üıyroid cancer. In: Thyroid
Disease Ed: Faik SA Lippincott Raven Philedelphia 1997;645-655.
2.
Schiumberger M and caillon B. Miscalaneous tumours
of the îhyroid. In The Thyroid Ed: Braverman LE, Utiger RD. Lippincott Raven,
Philadeiphia 1996;961-965.
3.
Aozasa
K, Inoue A, Tajima K, Miyauchi A, Matsuzuka F, Kuma K Malignant lymphomas of
the thyroid gland: Analysis of 79 patients with emphasis on histologic
prognostic factors. Cancer 1986;58(1):100-104.
4. Ansell SM, Grant CS,
Habermann TM. Primary thyroid lymphoma. Semin Oncol 1999;26:316-323.
5.
Freeman
C, Berg JW, Cutler SJ. Occurrence and prognosis of extranodal lymphomas. Cancer
1972;29(1):252-260.
6.
Canan Uzel, Yersu Kapran, G.rcan Vural, tarýk terzioûlu. Primary Thyroid
Lymphoma: A Report of Two Cases Turkish J Endocrinology and Metabolism 2002;1:41-45.
7.
Alzouebi
M, Goepel JR, Horsman JM, Hancock BW. Primary thyroid lymphoma: the 40 years
experience of a UK lymphoma treatment centre. Int J Oncol. 2012;40(6):2075-2080.
8.Derringer
GA, Thompson LDR, Frommelt RA, Bijwaard KE, Heffess CS, Abbondanzo SL.
"Malignant lymphoma of the thyroid gland: a clinicopathologic study of 108
cases. Am J Surg Pathol 2000;24(5):623-639.
9.Sippel
RS, Gauger PG, Angelos P, Thompson NW, Mack E, Chen, H. Palliative
thyroidectomy 110 for malignant lymphoma of the thyroid. Ann Surg Oncol 2002;9:907-911.
10.
Michels
JJ, C Delcambre, J Mamey. Et al. Lymphomes thyroidens primitils: étude
clinico-pathologique de 30 cas et revue de la littérature. Ann Pathol 2002;l22;10-17.
11.
Pederson R, Pederson N. Primary non-Hodgkin's Iymphoma 01 the thyroid gland: a
population based study. Histopathology 1996;28(1):25-32.
12.
Kossev P, Livolsi V. Lymphoid lesions of the thyroid: review in light of the
revised European-American lymphoma classification and upcoming World Health
Organization classification. Thyroid 1999;9(12):1273-1280.
13.
Derringer
GA, Thompson LD, Frommelt RA, Bijwaard KE, Heffess CS, Abbondanzo SL. Malignant
lymphoma of the thyroid gland: a clinicopathologic study of 108 cases. Am J
Surg Pathol 2000;24(5):623-639.
14.
Williams ED. Malignant lymphoma of the thyroid. C
Un Endocrinol Metabol 1Q 1981;379-389.
15.
Scholcfıeld JH, Quayle AR, Harris SC. Primary lymphoma of the thyroid the
association with Hashimoto's thyroiditis. Eur J Surg Oncol 1992;18(2):89-92.
16.
Rasbach
DA, Mend schein MS, Harris NL. Malignant lymphoma of the Lhyroid gland: A
clînical and pathologic study of twenty cases. Surgery 1985;98(6):1166-1170.
17.
Holm
LE, Blomgren H, Löwhagen T. Cancer risks in patients with chronic lymphocytic
thyroiditis. N Engl J Med 1985;312(10):601-604.
18.Moshynska
OV, Saxena A. Clonal relationship between Hashimoto thyroiditis and thyroid
lymphoma. J Clin Pathol 2008;61(4):438-444.
19.
Anscombe
AM, Wright DH. Primary malignant Iymphoma 01 the thyroid-a tumor 01
mucosa-associated Iymphoid tissue: review 01 seventy-six cases 1985;9(1):81-97.
20.
J Trotoux, D Aidan. Tumeurs du corps thyroïde. Encycl Méd Chir, ORL
2000;29(1):1-15
21.
Compagno
J, Celtel J. Malignant Iymphoma and other Iymphoprolilérative disorders 01 the
thyroid gland. A clinicopathologic study 01 245 cases 1980;74(1):1-11.
22.
N
Ibnou Souliane, A Chadli, H El Ghomari. Et al. Lymphome malin primitif de la
thyroïde 2002;63(3):231-234.
23.
Burke
JS, Butler JJ, Fuller LM. Malignant lyrnphomas of Ihe thyroid: A clinical
pathologic study of 35 patients inclııding uhrastructurae obscrvations. Cancer 1977;39(4):1587-1602.
24. Ravinsky E, Morales C. Diagnosis of
lymphoma by image-guided needle biopsies: Fine needle aspiration biopsy, core
biopsy or both? Acta Cytol 2005;49(1):51-57.