A Systematic Review on Renal Transplantation: Is Quality of Life Compromised After Transplantation
Keywords: Kidney transplantation; Renal transplant; Quality of life; Well-being
The two most common causes of renal failure are hypertension and diabetes. Additional causes of chronic kidney disease (CKD/ESRD) can be categorized as intrinsic renal (glomerulonephritis, focal-segmental glomerulosclerosis), postrenal (obstacle, reflux nephropathy), or prerenal (chronic or acute ischemia). Kidney transplant candidates are those with a glomerular filtration rate (GFR) of less than 30 mL/min/1.73 m, also known as stage 4 chronic kidney disease (CKD)7 The only effective treatment for end-stage renal disease is kidney transplantation, which can improve the quality of life for the majority of patients by addressing metabolic, haematological, endocrine, and immune system problems in addition to the illness's immunological function. Medical knowledge and technology have advanced in this area, yet issues still exist that limit the number of successful transplants performed. One of the biggest challenges, aside from the dearth of organs donated by live or deceased donors, is managing the pre- and post-transplant routes, which are frequently solely medical-surgical and ignore the significance of maintaining bodily and mental integrity. Rapid anatomical and physiological functioning is made possible by surgery in transplantation; nevertheless, cognitive and emotional integration is also required. A surgical procedure like a transplant involves a lot of stress, which puts one's continuity and integrity at risk. It also elicits strong emotions and has the potential to change a person's identity by generating psychopathology and psychosocial issues8-12. Haemorrhage, Thrombosis, Infection, Arterial Stenosis, Lymphocele, Urinoma, graft rejection and even skin cancer can occur as a complication of this transplantation13.
The schematic representation of kidney transplants is shown in the (Figure 1)14.

Figure
1.
This figure shows a transplanted kidney.
Even with all of the risks, there is a significant chance that this
transplant will save the patient's life. There are legitimate benefits,
however, there are concerns over the quality of life following the transplant. The multifaceted
idea of quality of life (QoL) refers to a person's overall state of well-being
concerning the values, surroundings, cultural context, and social environment
in which they live. Since QoL assesses factors other than bodily functioning
and morbidity, it is acknowledged as a crucial indicator of overall15. According to the study, cultural factors,
personality traits of both patients and the relationship between the donor and
recipient may all have an impact on the experience of psychopathological
symptoms. In the US, anxiety and mood disorders affect 18.1% and 9.5% of adults
annually, respectively. They have been connected to higher rates of disability,
non-compliance, acute sickness, exacerbations of chronic illness, and even
death in post-transplant individuals. Depression and anxiety are common ailments
in the general public. In Nepal, 2100 adults between the ages of 18 and 65
participated in a nationwide cross-sectional study. The results showed that the
quality of life was negatively correlated with the age and gender-adjusted
point prevalence of anxiety (16.1%), depression (4.2%), and combined
comorbidity (5.9%)16.
There are further studies have found that post-transplantation is
associated with a higher rate of depression which would decrease the QoL
post-transplantation. Although surgical techniques have consistently
improved, therapeutic targets for preventing graft rejection have been
identified, and post-transplant complications have decreased, there are still
many unanswered questions and it is unknown how much the quality of life has
been affected by transplantation. Furthermore, the general public is ignorant of
ways to enhance the quality of life following a transplant. For the reasons
outlined above, we conducted a thorough literature search to determine the
association between quality of life and kidney transplantation and to provide a
comprehensive understanding of this in this systematic research.
3. Materials and methods
3.1
Reporting Guidelines
This
systematic research aims to identify if the quality of life is compromised in a
patient’s post-renal transplant. This systematic review has been conducted
according to the Preferred Reporting Items for Systematic Reviews and
Meta-Analyses (PRISMA) 2020 guidelines17. As secondary data from published articles were used, ethical
approval was not considered.
3.2 Search Strategy
The
search was conducted online on PubMed, Google Scholar, Science Direct, BMC, and
Cochrane. The last search on all databases was on November 29, 2023. Keywords
that have been utilized for the websites include kidney
transplantation,” “renal transplant”, “quality of life”, and “well-being. Keywords presented in this systematic review were
targeted by Medical Subject Headings search (Mesh). The Boolean
method was used to combine the keywords to create a uniform search through the
various databases mentioned above. We identified 4983 potentially eligible
records across all the databases. Different search strategies used in various
journals have been summarized in (Table 1).
Table
1. A summary of search strategies
used in Pubmed, google scholar,cochrane,BMC
and science Direct.
and science Direct.
|
|
Key word |
Result |
Filter Used |
Search Strategy |
|
PUBMED |
“Kidney
transplantation,” “renal transplant”, “quality of life”, “well-being” |
1045 |
2013-2023 |
kidney
transplant or renal transplantation OR(( "Kidney
Transplantation/classification"[Mesh] OR
"Kidney Transplantation/ethics"[Mesh] OR "Kidney Transplantation/history"[Mesh]
OR "Kidney
Transplantation/methods"[Mesh] OR
"Kidney Transplantation/mortality"[Mesh] OR "Kidney
Transplantation/psychology"[Mesh] OR
"Kidney Transplantation/rehabilitation"[Mesh] )) OR (
"Kidney Transplantation/adverse effects"[Mesh] OR "Kidney
Transplantation/education"[Mesh] OR
"Kidney Transplantation/instrumentation"[Mesh]OR "Kidney Transplantation/statistics and
numerical data"[Mesh] OR
"Kidney Transplantation/trends"[Mesh] ) AND quality of life
or well-being or (( "Quality of Life/legislation and
jurisprudence"[Mesh] OR
"Quality of Life/psychology"[Mesh] )) AND
"Socioeconomic Factors/history"[Mesh]
|
|
Google scholar |
“Kidney transplantation,” “renal
transplant”, “quality of life”, “well-being” |
237 |
Advanced
search with all the keywords only in the title |
Renal transplantation, Quality of life |
|
Cochrane |
“Kidney transplantation,” “renal
transplant”, “quality of life”, “well-being” |
66 |
No filter used |
Renal transplantation, Quality of life |
|
BMC |
“Kidney transplantation,” “renal
transplant”, “quality of life”, “well-being” |
249 |
2022-2023 |
Renal transplantation, Quality of life |
|
Science Direct |
“Kidney transplantation,” “renal
transplant”, “quality of life”, “well-being” |
3386 |
No filter used |
Renal transplantation, Quality of life |
t.
3.4 Inclusion Criteria
The systematic review's inclusion criteria encompassed research that juxtapose quality of life (QoL) with renal transplantation. The population of the studies was not restricted based on gender or ethnicity. We limited our search to English-language records published online between November 29, 2013, and November 29, 2023, that are freely downloadable full texts and include participant identities. The investigation also includes literature, systematic reviews, observational studies, meta-analyses, and randomized controlled trials (RCTs).
3.5
Exclusion Criteria
Excluded
from consideration were articles published before 2013, case reports,
unpublished publications, editorials, publications written in languages other
than English, and studies using animals or patients younger than nineteen. The
population, intervention, comparison, and outcomes (PICO) criteria served as
the foundation for our inclusion criteria.
3.6
Data Selection and Extraction
The
first and second authors, who are distinct individuals, chose and extracted the
pertinent studies on their own. Talking about the study's design, the
intervention that was used, the results that were measured, and how these
related to our inclusion and exclusion criteria, the two researchers agreed on
eligibility criteria. After duplicates were eliminated using EndNote
(Clarivate, Philadelphia, PA) software, 71 articles were chosen from the five
databases. Using the search technique and the inclusion and exclusion criteria,
we found articles that were directly connected to the topic at the start of the
screening process. After the articles were screened and examined by the
researchers, 27 were chosen for quality assessment. These 27 were chosen for a
quality assessment screening.
3.7
Quality Assessment
The 27 chosen
articles are then assessed by two authors (the first and second authors) using
tools such as the Newcastle-Ottawa Scale adapted for cohort and case-control
studies, The SANRA (scale for the assessment of narrative review articles)
checklist for review articles18,19
and JBI (The Joanna Briggs
Institute Critical Appraisal Tools) for case reports. Two authors
investigated the risk of bias using tools. Each study was assessed by these
tools and scored accordingly. Studies with a minimum accepted scoring of
>70% in checklists were selected. This selection has been briefly summarized
in (Table 220-31and
Table 332).
Table 2. The selected articles after quality appraisal, SANRA,
the scale for the assessment of narrative review articles
|
Studies selected after
review |
Study type |
Quality appraisal tool |
Total score of the tool |
Acceptable score |
|
Tessa. S. S et al |
Systematic review |
SANRA |
12 |
8 |
|
Vivian. V et al |
Cross-sectional study |
Newcastle-Ottawa scale |
9 |
7 |
|
Chilcot et al21 |
Review article |
SANRA |
12 |
8 |
|
ShiMin Hu et al |
Cross-sectional study |
Newcastle-Ottawa scale |
9 |
7 |
|
Masud.I et al |
Cross-sectional study |
Newcastle-Ottawa scale |
9 |
7 |
|
Megawati et
al |
Cross-sectional study |
Newcastle-Ottawa scale |
9 |
7 |
|
Naafiah
K.M |
Cross-sectional study |
Newcastle-Ottawa scale |
9 |
7 |
|
Eliza et al |
Cross-sectional study |
Newcastle-Ottawa scale |
9 |
7 |
|
Vinke JSJ et al27 |
Review article |
SANRA |
12 |
8 |
|
Jordakieva G28 |
Cross-sectional study |
Newcastle-Ottawa scale |
9 |
7 |
|
Marcin P et
al |
Review article |
SANRA |
12 |
8 |
|
Overbeck I et al |
Cross-sectional study |
Newcastle-Ottawa scale |
9 |
7 |
|
Pasquale, et al |
Cross-sectional study |
Newcastle-Ottawa scale |
9 |
7 |
Table
3. The selected articles after quality appraisal, JBI (The Joanna Briggs
Institute Critical Appraisal
Tools)
|
Studies selected after review |
Study type |
Quality appraisal tool |
Included /Excluded |
|
Witmanowski, H et al33 |
Case report |
JBI Critical Appraisal Checklist for Case Reports |
Included |
4. Results
A QoL and renal transplantation groups were screened
for in all five databases. First, we used the search results to find papers.
Our search was narrowed down to 4983 publications after we used several
restrictions, including the English language, free-full text, keywords in the
title, and our inclusion/exclusion criteria. The EndNote software (Clarivate,
Philadelphia, PA) removed 877 duplicates before the studies were selected and
reviewed. To ascertain whether the titles and abstracts of the 870 papers were
relevant to our review, they underwent a thorough evaluation. 799 of the
screened items were removed because they didn't fit the topic, goals,
inclusion, or exclusion criteria. As a result, 27 papers were selected for
eligibility verification and quality assessment. This procedure is illustrated
in full in (Figure 2)
of the PRISMA flowchart.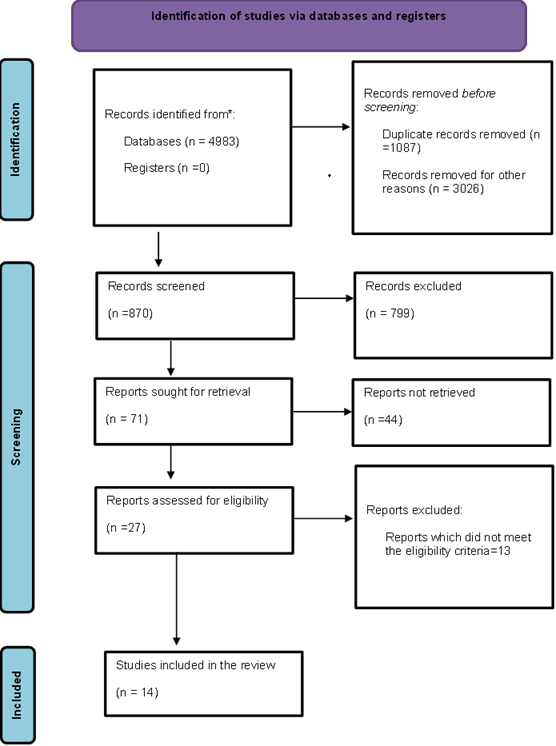
Figure 2. Flowchart of the PRISMA PRISMA: Preferred Reporting Items for Systematic Reviews and
Meta-Analyse A total of 14 articles made it to the final review20-32. (Table 4) contains the details of the relevant 14 articles included20-32. Table 3. Details of the relevant 14 articles after quality appraisal
5. Discussion With the evolution of the modern era in medicine and surgery, End-stage
renal disease hasfound an alternative treatment with renal transplantation. As
their renal function gradually declines, individuals with chronic kidney
disease (CKD) experience a degradation of their quality of life (QOL) as well
as an increased risk of morbidity and mortality. Patients with chronic kidney
disease (CKD), which includes those receiving dialysis, bear heavy physical and
psychological loads such as fatigue, pruritus, insomnia, pain, sadness, and
restless legs syndrome. These conditions eventually deteriorate physical and
psycho-social health. For these populations, renal transplantation will be a
lifesaver. Several studies have explained the uses of renal transplantation in
recent days. The main goal of this treatment is to provide an increased
survival rate and quality of life. The studies evaluated in this systematic
review have another aspect of renal transplantation in satisfying the quality
of life. This research focuses on the various advent events to be faced after
the surgery and provides a clear view of how the quality of life is affected. 5.1 Psychological reliability This is the ability of a person to perform professional activities in
difficult and extreme situations as successfully as under normal conditions is
frequently associated with the notion of psychological stability.32 5.2 Mentel Distress Pasquale, et al study explains that for end-stage kidney disease,
kidney transplantation is a proven treatment. Nonetheless, it is a complicated
psychological experience that may result in psychopathology and mental anguish.32 5.3 Depression Feelings and Intellectual Problems Research on the cognitive abilities of kidney transplant recipients has
revealed cognitive deficits, particularly in verbal memory and executive
function-disabilities that are frequently linked to mood problems. Cognitive
Impairments and Depression Symptoms: These negative effects can linger and
negatively affect all facets of life.29,32 5.4 Depression, anxiety, and sleep disorders After receiving a kidney transplant, patients frequently experience
poor sleep, which is one of the things that negatively impacts their quality of
life. This issue is linked to both a higher level of medical comorbidity and
emotional fragility27,30,32. According to Vivian et al study's findings, anxiety raises the
likelihood that transplant recipients would experience depression and
significantly predicts its severity. Furthermore, we discovered that the
perception of inadequate social support was linked to a higher chance of depression.
This finding is in line with earlier research showing that social
support-related factors, such as living alone, having a less supportive family
environment, and having lower marital satisfaction, are strongly associated with
an increased risk of depression in patients undergoing renal transplantation
and end-stage renal disease21. ShiMin Hu et al findings
demonstrated that patients' capacity for self-management, particularly in the
psychosocial domain, could be severely compromised by both depression and
anxiety. The general patient data from this investigation, as well as the
associations between anxiety and depression and the capacity for
self-management and endogenous creatinine clearance, were examined23,26. Even with improvements in kidney transplantation, depression is still a
common and troublesome comorbidity that is often disregarded. In this context,
depression is associated with poor outcomes, such as lower graft survival.
Although more empirical research is needed to fully understand the mechanisms
underlying this association, nonadherence is a major explaining factor22. 5.5 Employment status: Eliza et al research concluded that the employment status has the
lowest mean after the transplantation which means the employment status is
affected after renal transplantation27,32. On the other hand,
Jordakieva et al states that there is good employment in post-transplantation
individual which is controversial29. According to certain other
research, kidney transplants improve life quality20,24,25,31. 5.6 Anaemia: Kidney transplant recipients (KTRs) have a significant prevalence of
iron insufficiency (ID), which has been independently linked to an increased
risk of death28. The possible mechanism of iron deficiency in renal
transplant is postulated in (Figure 3).
|