A Twist of Fate: Spontaneous Closure of a Dural AV Fistula
Abstract
Dural arteriovenous
fistulas (DAVFs) are rare vascular malformations characterized by abnormal
connections between dural arteries and venous sinuses or cortical veins, with
clinical presentation ranging from benign symptoms to seizures or hemorrhage1.
We report a case of a
35-year-old male who presented with a generalized tonic-clonic seizure.
Magnetic Resonance Imaging (MRI) of the brain showed findings suggestive of an
arteriovenous malformation. This was subsequently confirmed by digital
subtraction angiography (DSA) as an anterior cranial fossa DAVF with cortical
venous drainage, typically considered high risk. The patient was scheduled for
endovascular embolization; however, during the procedure, no evidence of the
fistulous connection or early venous drainage was identified. Follow-up imaging
confirmed the spontaneous closure of the DAVF. Spontaneous regression of DAVFs
is a rare occurrence, particularly in high-grade lesions and may be attributed
to post-angiographic thrombosis, hemodynamic shifts or natural vascular
remodelling2. This case reiterates the importance of re-evaluating
patients prior to treatment, especially when there is a time lag between
diagnosis and intervention. It also emphasizes the need for ongoing
surveillance as there is always a potential risk of recurrence.
Keywords: Dural arteriovenous fistulas; Magnetic Resonance
Imaging; Digital subtraction angiography
Introduction
Dural AV Fistulas are
abnormal shunts between dural arteries and dural venous sinuses or cortical
veins3. Their presentation ranges from benign symptoms like
headaches to serious outcomes such as seizures or intracranial hemorrhage.
Spontaneous closure of DAVFs is rare but recognized, typically associated with
changes in hemodynamics or post-procedural effects4. This case highlights such an unexpected resolution.
Case
Presentation
A 35-year-old male, chronic
alcoholic, presented with a generalized tonic-clonic seizure following binge
drinking. On examination, patient was conscious and oriented with Glasgow coma
scale (GCS) E4V5M6 and no neurological deficit. His laboratory investigations
were unremarkable. He was started on anti-epileptic medications.
Magnetic Resonance (MR) Brain was
performed which was suggestive of few prominent flow voids in the sulcal spaces
in left frontal region with mild parenchymal edema in the adjacent frontal
lobe, suggestive of an arteriovenous malformation (Figure 1 A-F).
A digital subtraction angiography
(DSA) was performed for further evaluation. Right femoral access was taken with
a 5F short sheath. Selective catheterization was done and contrast was injected
into the bilateral common carotid arteries, internal and external carotid
arteries and vertebral arteries and images acquired. These revealed an anterior
cranial fossa DAVF with arterial feeders from the posterior ethmoidal branch of
the right ophthalmic artery and orbitofrontal branch of the left ACA. The
fistula drained directly into an ectatic cortical vein. No feeders could be
identified from either ECA or left ophthalmic artery (Figure 2 A & B).
The patient was advised fistula closure by endovascular embolization.
After a few days the patient was
admitted for embolization under GA. Right CFA access was taken with 6 F short
sheath using Envoy 5F guide catheter and wire combination, right ICA gram was
obtained. 2mg infusion of Nimodipine was started slowly. Using marathon
microcatheter and mirage microwire combination, right ophthalmic artery was
cannulated. Fistulous branches were cannulated with marathon micro-catheter
taken over mirage 0.08” microwire till the dural AVF nidus.
No early draining veins or fistulous
connection was observed despite super selective catheterization.
Super-selective cannulation of the right ACA was done however no early draining
veins were found. Normal filling of intracranial circulation was seen (Figure
3 A-C). Contralateral ICA injection confirmed spontaneous closure of the
DAVF (Figure 3D).
Figure 1: (A) - T2W coronal image showing hyperintense signal
with a focus of hypo intensity within in left frontal region (ARROW)
(B) - SWI showing a
prominent draining vessel in left frontal region (ARROW)
(C), (D) and (E) - 3D
FLAIR images in all planes showing prominent flow void with mild parenchymal
edema in left frontal region (ARROW)
(F) - ASL images
showing hyper perfusion in the affected area (ARROW)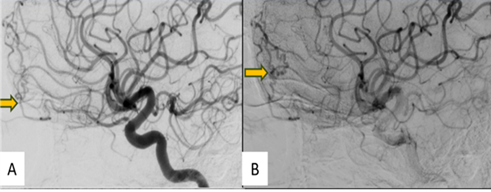
Figure 2: (A) &(B) - Digitally
subtracted images through the right internal carotid artery showing anterior
cranial fossa DAVF with arterial feeders from the posterior ethmoidal branch of
the right ophthalmic artery and orbitofrontal branch of the left ACA (arrow)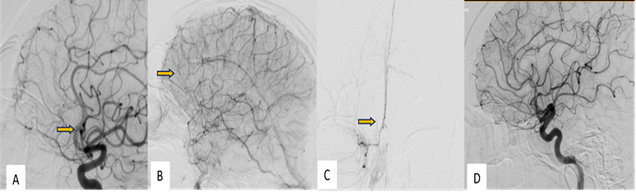
Figure 3: (A), (B) Selective digitally
subtracted angiography images in arterial and venous phases through the right
Internal Carotid Artery did not show any fistula at the previously documented
site (arrow)
(C) - Superselective digitally
subtracted angiography images through the branches of anterior cerebral artery
did not any fistula (arrow)
(D)- Selective digitally
subtracted angiography images through the contralateral (left) Internal Carotid
Artery did not show any fistula at the previously documented site
Discussion / Summary
DAVFs represent
abnormal vascular communications between meningeal arteries and dural venous
sinuses or cortical veins2. While they account for only 10-15% of
intracranial vascular malformations, their clinical presentation and potential
for serious complications-such as intracranial hemorrhage, seizures or
progressive neurological decline make early diagnosis and management critical5.
The Cognard
classification system is a widely used grading system for dural arteriovenous
fistulas (DAVFs). It categorizes these vascular abnormalities based on their
venous drainage patterns and clinical implications6.
In the present case,
the patient exhibited a DAVF located in the anterior cranial fossa with
cortical venous drainage, which typically confers a higher hemorrhagic risk as
per the Cognard classification (Grade III or IV). Prompt endovascular or
surgical intervention is usually indicated in such high-grade lesions1. However, this case
took an unexpected turn when the DAVF demonstrated spontaneous angiographic
resolution just days after diagnostic workup and prior to embolization-highlighting
a rare but well-documented phenomenon in neurovascular literature1.
Four primary
mechanisms have been proposed to explain the spontaneous closure of DAVFs:
post-angiographic thrombosis, hemodynamic alterations, venous remodelling and
fibrosis and natural healing and immune response1.
• Spontaneous thrombosis: Thrombosis can occur within a dural arteriovenous fistula (DAVF), often due to changes in blood flow dynamics, leading to reduced or ceased blood flow.
• Hemodynamic influences: Variations in systemic blood pressure, local vascular resistance and vascular remodelling can alter hemodynamics, potentially facilitating the spontaneous closure of the DAVF over time.
• Venous remodelling: Remodelling of the venous drainage pathways associated with the DAVF is another proposed mechanism. As the venous drainage pattern adapts to accommodate altered hemodynamics or increased venous pressure due to the fistula, it may lead to progressive narrowing or closure of the abnormal connection. This venous remodelling process could be influenced by changes in vascular endothelial integrity, collagen deposition or fibrotic changes within the venous walls.
• Natural healing processes: The body's innate healing mechanisms, including local inflammatory responses, tissue repair processes and vascular remodelling mechanisms, may also contribute to spontaneous closure of DAVFs. These mechanisms may act independently or in combination, with each potentially influencing the others in a given case. Recanalization of the occluded draining sinus could prompt regression of the dAVF7. Indeed, some authors have claimed haemorrhage could trigger the closure of intracranial arteriovenous malformations8. Although various factors may contribute to spontaneous closure, its occurrence and timing remain unpredictable. This underscores the importance of re-evaluating fistulas prior to treatment, especially if a delay occurs and maintaining follow-up due to the potential risk of recurrence3.
In our case, the patient’s DAVF may have
closed due to altered hemodynamics or spontaneous thrombosis following
diagnostic angiography.
Conclusion
DAVFs carry variable prognoses
depending on their drainage pattern and location. While interventional therapy
remains the mainstay of treatment, spontaneous resolution is a recognized rare
outcome. This case reiterates the importance of follow-up imaging and clinical
reassessment before planning invasive procedures.
References
1. Al-Afif S, Nakamura M, Götz F, Krauss JK. Spontaneous
closure of a dural arteriovenous fistula. BMJ Case Rep 2014;2014:2014011255.
2. Luciani A, Houdart E, Mounayer C, Saint Maurice JP,
Merland JJ. Spontaneous closure of dural arteriovenous fistulas: report of
three cases and review of the literature. AJNR Am
J Neuroradiol 2001;22(5):992-996.
3. Baldazzi
D, D’Andrea V, Bernetti C, et al. Predictive factors for spontaneous resolution of dural
arteriovenous fistulas: a systematic review. J Med Imaging Interv Radiol
2024;11(1).
4. Hansen JH, Søgaard I. Spontaneous regression of an
extra- and intracranial arteriovenous malformation: Case report. J Neurosurg
1976;45(3):338-341.
5. Saini J, Beniwal M, Somanna
S, et al. Spontaneous Closure of Dural Arteriovenous Fistula; A Visual Specter.
Neurol India 2019;67(5):1376.
6. Gandhi D, Chen J, Pearl M, Huang J, Gemmete JJ,
Kathuria S. Intracranial Dural Arteriovenous Fistulas: Classification, Imaging
Findings and Treatment. Am J Neuroradiol 2012;33(6):1007-1013.
7. Saito A, Furuno Y, Nishimura S, Kamiyama H, Nishijima
M. Spontaneous Closure of Transverse Sinus Dural Arteriovenous Fistula - Case
Report. Neurol Med Chir 2008;48(12):564-568.
8. Abdulrauf SI, Malik GM, Awad IA. Spontaneous Angiographic
Obliteration of Cerebral Arteriovenous Malformations. Neurosurgery
1999;44(2):280-287.