A Very Extensive Cholesteatoma Complicated by Facial Paralysis and Bezold Abscess
Abstract
Introduction: bezold’s abscess is a rare complication of chronic otitis media, and it can be life-threatening with its insidious onset. Treatment consists of urgent surgical debridement and a long course of antibiotics.
Case presentation: we present a case of a 45-year female admitted to our department for a long-neglected otorrhea of the right ear complicated with facial palsy, mastoiditis, and two cervical fistulas; the patient presented a cophosis on the right side with grade vi facial palsy. Temporal bone ct scan showed a right filling of the middle ear with complete erosion of the mastoid cells, ossicular chain, and facial canal and extended erosion of the inner ear. The patient underwent a right canal-wall-down mastoidectomy, which showed destruction of the ossicular chain, the vii nerve canal, the lscc, the vestibule, and the cochlea with an excision of the fistulous tract of the ancient bezold’s abscess.
Discussion: it is rare to find ba (bezold’s abscess) as the first otologic manifestation of chronic otitis media. Otalgia, otorrhea, and painful lateral neck swelling with postauricular fluctuance are the main clinical findings. Temporal ct scan and mri normally show an abscess of the upper neck, which communicates with the destructed mastoid cavity via the eroded mastoid tip. Treatment consists of using intra-venous broad-spectrum antibiotics and surgical mastoidectomy with possible drainage of the abscess by trans mastoid approach.
Conclusion: bezold abscess is a complication of mastoiditis that is rarely seen in daily practice since the regular use of antibiotics. The collection can fistulize to the skin if non-treated, which was seen in our patient. Treatment consists of surgical debridement and a long course of antibiotics
Keywords: bezold abscess; cutaneous fistula; mastoiditis
Introduction
Chronic
otitis media is commonly viewed in our day-to-day ent consultations, but it is
rare to see many complications in one patient. Bezold’s abscess is an
infrequent complication of mastoiditis1.
The diagnosis’s delay due to the initial unharming presentation can lead to
life-threatening situations2. The
surgical treatment consists of debridement of infected tissues and a long
course of antibiotics.
Case
presentation
It
is a case of a 45-year-old female admitted to our department for right chronic
otorrhea with no significant surgical or medical history. The onset of the
symptomatology goes back to childhood, with the patient having a right
persistent purulent otorrhea complicated with facial palsy, mastoiditis,
hypoacusis, and recurrent spells of vertigo. The medical examination found a
healthy woman in a good general state; the temperature was at 37,4 celsius, and
there were no anterior spells of headaches, vomiting, blurry vision, or any
signs of intracranial hypertension. An otoscopy of the right ear exhibited
stenosis of the right external auditory canal with an associated polyp blocking
the exploration of the tympanic membrane. The left ear showed a non-marginal anterior
perforation. An active retro auricular fistula orifice issuing pus on the right
side was noted, and a second sequalae fistula orifice was also noted inferior
to the precedent in the right spinal region. A complete right-sided peripheral
facial palsy was also noted. The vestibular examination showed a grade 3
spontaneous left nystagmus and right swaying on the romberg and the fukuda
examination. The neurological examination showed no other cranial palsies and
no motor or sensory deficit. A pure tone audiogram showed right-side cophosis
and left-side sensory-neural hearing loss with an average threshold of 55 db
and an a-b gap of 15 db. A temporal bone ct scan showed a right filling of the
middle ear with complete erosion of the mastoid cells, ossicular chain, and
facial canal, and extended erosion of the inner ear. A vhit was demanded,
exhibiting a unilateral right vestibular loss with many covert saccades in the
middle eye traces. The bezold’s abscess diagnosis was retained, and the patient
was hospitalized and put on a long course of intravenous antibiotics and local
treatment and toilet of both ears for 15 days. In the third week, the patient
underwent a right canal-wall-down mastoidectomy, which showed destruction of
the ossicular chain, the vii nerve canal, the lscc, the vestibule, and the
cochlea with an excision of the fistulous tract of the ancient bezold’s
abscess. The patient continued another five days' courses of intravenous
antibiotics and dressing replacement every day, and the patient was released on
the eighth day.
Discussion:
Bezold’s
abscess (ba) is an intratemporal complication of mastoiditis that occurs when
the infection surpasses the mastoid cortex laterally and goes medially to the
attachment of the sternocleidomastoid muscle3.
The regular use of antibiotics had a considerable impact on the number of cases
of ba, with a significant decrease3.
It is rare to find ba as the first otologic manifestation of chronic otitis
media. Otalgia, otorrhea, and painful lateral neck swelling with postauricular
fluctuance are the main clinical findings4
our patient did not have neck swelling at presentation due to the fistulization
of the abscess to the skin. Many studies concluded that cholesteatoma was the
main otitic condition underlying in patients with extracranial and intracranial
complications with a percentage of 53-78,5%5-9.
Temporal ct scan and mri normally show an abscess of the upper neck, which
communicates with the destructed mastoid cavity via the eroded mastoid tip5.
Treatment
consists of using intra-venous broad-spectrum antibiotics, surgical
mastoidectomy with possible drainage of the abscess by trans mastoid approach10, and debridement of the granulation tissue6. In our case, the abscess fistulized to the
skin; that’s why we did not drain it surgically (figure 1,2,3,4,5 and 6).
Figure
1.
Image showing a right retro auricular and spinal region cutaneous fistula
confirming the outcome of the bezold’s abscess.
Figure 2. Image showing a right peripheral facial palsy
stage v on the house-brackmann classification. 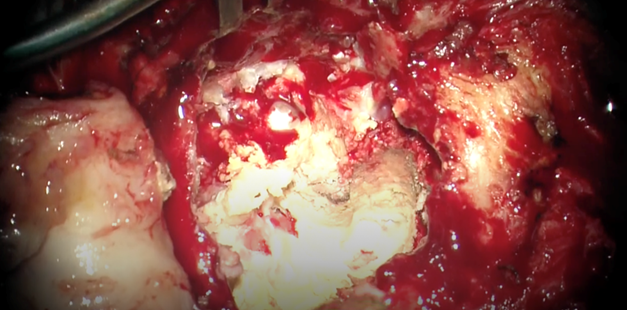
Figure 3. Operative image showing the extension of the
cholesteatoma and erosion of the mastoid and middle ear structures. 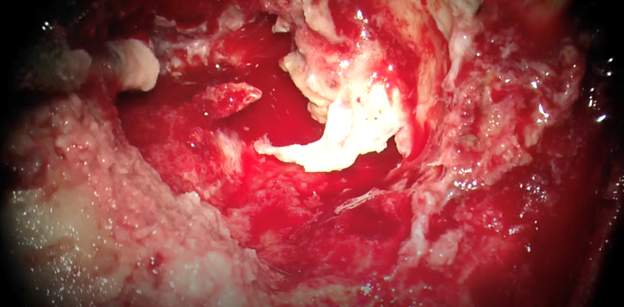
Figure 4. Operative image
showing the erosion of the fallopian canal and the facial nerve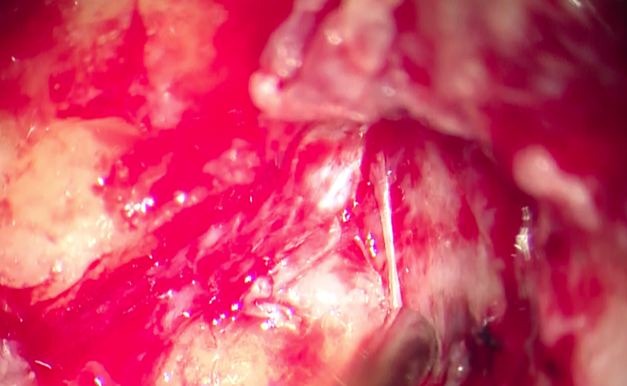
Figure 5. Operative image showing invading the carotid canal
and jugular gulf.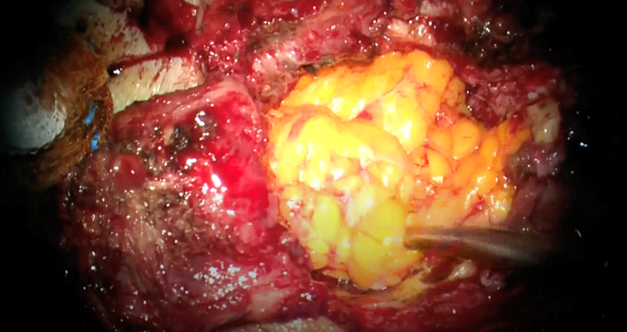
Figure 6. Filling of the remnant cavity with abdominal fat.
Conclusion:
Bezold
abscess is a complication of mastoiditis that is rarely seen in daily practice
since the regular use of antibiotics. The collection can fistulize to the skin
if non-treated, which was seen in our patient. Treatment consists of surgical
debridement and a long course of antibiotics
References:
2.
lin h, lin y. Bezold abscess. Ear,
nose & throat journal 2015
3.
winters
r, hogan cj, lepore ml, geiger z. Bezold abscess. Statpearls 2023.