Adding A Perspective to The Clinical Problems of C-PTSD
Introduction
Several
years ago, a patient was referred to me from a clinic i work with. No
forwarding information, however. When
mr. C showed up in my office, i met a man who is probably the most traumatized
patient i have ever worked with. During our first session he was at times
incoherent and rambling, appearing totally uncomfortable about just being
alive. Eventually, with time and
patience on my part, he began to tell his story.
He related
that he had a “pretty normal life” growing up with his older sister and two
parents, until about the 6th grade.
Somewhere in that year his father found out that his mother had been
embezzling money from her work. A lot of
money. The family had a rather rich
lifestyle as a result. But then
everything went downhill rapidly. His
father became unglued and abused. He turned out to be a very sadistic man in
the treatment of his 2 children. Overnight, mr. C’s life because an unending
nightmare. He survived by burying himself in school and sports. He became a straight-a and a track star. Nonetheless, he had to internalize a
tremendous amount of trauma from his life at home. His home life was filled with abuse,
uncertainty, chaos, disappointments, constant stress, sleepless nights, fear,
heightened anxiety and depression, along with a father whose behavior was
becoming increasingly sadistic. Amazing that he survived.
At the time
he came to see me, he was reliving a fight to the death with father one year
previous. Over time we came to understand (the importance of the doctor-patient
relationship) that this fight with his father had been a fight for his very
survival. He now understood that his father had intended to kill him, and that
he had barely survived as he was fighting him off. What does anyone do when they realize that
their very own parent wants them dead!
by the end of that first session, i had
concluded that mr. S was experiencing a “shock trauma”. In this state, his condition was identical to
his having been involved in a car accident, a military incident, as a customer
in a bank robbery, or a climate disaster.
Now
what? I concluded that mr. C was a
prisoner of that traumatic experience and the past traumas he was forced to
endure. What does this mean: a prisoner
of his experience? This is what
complex-ptsd is all about.
C-ptsd
C-ptsd can best be defined in terms of the following:
Intrusive
experiences: this includes re-experiencing trauma from the past, flashbacks,
recurrent memories, and nightmares.
Persistent
avoidance: this includes avoiding all thoughts, feelings, objects, people, and
places associated with traumatic events.
Negative
changes in cognition and mood: this would include distorted beliefs about self and the world
around them. Persistent feelings of
shame and guilt. Emotional numbing. Feelings
of alienation and the desire to be isolated and withdrawn from others.
Alterations
in arousal and reactivity: this includes an increase in irritability and hypervigilance,
tendencies toward reckless behavior, sleep disturbances, and difficulties with
focus, attention span, and concentration.
Dissociation: this occurs unconsciously when a
person is overwhelmed by internal or external stimulation. The mind just goes
elsewhere than where the person’s body is for protection.
Recent thinking about c-ptsd considers that the best definition of
this diagnosis includes when a person becomes a prisoner of their experience1. Examples would be prisoners of war, human
trafficking, kidnapping, cruel work experiences when you absolutely have to
have this job. Over time i came to understand that mr. C felt a prisoner of
long-term trauma with his father.
The course of treatment
As
our work progressed over 2 years, several other factors began to appear. After
working for a number of years to free himself of all the trauma and abuse he
experienced from his father, everything collapsed, and he was right back at
square one. He had built a strong relationship with a wonderful woman and was
looking forward to spending his life with her. However, his parents, although
separated at the time, had another child while his father was living on the
streets and his mother was unemployed. Very quickly this burden fell on my
patient, and he was once again immersed in chaos, abuse, and craziness taking
care of his mother until she was able to get back on her feet. His girlfriend couldn’t cope with the added
chaos and craziness, and she left. All of this was devastating to mr. C.
Secondly,
mr. C increased his alcohol use. Sadly, he gave up sports for alcohol. By the
second year of our work together his liver enzymes came back abnormal. Which he
mentioned did not bother him all that much, because hard alcohol use was
serving a purpose for him. He noted that his alcohol use was getting rid of his
flashbacks. And that this was a big deal
for him, not having to deal with daily flashbacks in his mind. This was a very
disruptive experience for him, which is why he continued to use alcohol. However, the risky consequences of this choice
were becoming apparent.
Third,
i have the observation that trauma always gets imprinted into the neurological
circuitry of the brain. And it is there
permanently to remind the individual not to go there again! But what happens to
this individual when their brain/mind is carrying this burden. As my patient
expressed to me, he struggles with this almost every moment of every day. Is it
a great credit to him that despite this burden he remains a straight a college
student, and he cares for his new bother as a father would. But again, he is paying a price as
demonstrated by his abnormal liver enzymes.
Which brings back to this is how his brain is wired. And how do we change this?
Imprinted
The person’s brain/mind becomes preoccupied with their past traumas, and this interferes with their present, daily lives. Exactly what mr. C had related to me. Everyday he had to struggle with constant flashbacks and memories of his past. It is amazing that he was able to accomplish as much as he did. But again, at a huge cost. As long as he was able to use alcohol, he could numb the traumas and escape the flashback, memories and nightmares, temporarily. While at the same time, his liver was being poisoned.
In looking around at the mental health field, i observe that cognitive-behavioral therapies attempt to change the patient’s thinking and therefore their behavior. My concern is that this doesn’t work well enough because the damage is imprinted into the neurological circuitry of the brain. We must address how deeply the brain responds to trauma, and not just address treatment at the psychological level.
Healing
In
my experience, it is the doctor-clinician relationship that is the key to
healing trauma. Below is a small example of our work together.
(p) “i used to think that my
life had been totally derailed and that i would never be able to get my life
back on track. But from our work together i can see that it wasn’t being
derailed that
was central to my life, it was tough competition”.
(d) “what exactly do you mean by
tough competition? Are you referring to the struggle for everyday survival?”
(p) “yes! It was being able to
survive everyday that took all my energy. This is what was always in the way of
getting to my destination and achieving my destiny”.
(d) “do you feel that you are on
the right road now? That are finally going to be able to beat the competition
and leave this awful “prison of trauma behind”?
(p) “yes! But i believe there is still more work to be
done”.
(d) “i agree”.
In
part ii of this article (coming soon), i will address how we can rewire the
neurological circuitry of the brain that has imprinted these traumatic
experiences. And no, this is not easy work for either the patient or the
clinician.
Summary
The
literature i have reviewed does recognize that ptsd and c-ptsd affect brain
functioning. This research has demonstrated that ptsd rewires the brain’s
information processing system leading to difficulties interpreting
non-threatening stimulation as threatening. And demonstrating that ptsd causes
significant impairments with emotional regulation, relationships with others,
self-identity, and fragmentation of the self.
The most prominent effects occur in the amygdala (raising fear and
anxiety), hippocampus (affecting the laying down of memories), and the pfc
(pre-frontal cortex) with disturbances in cognition and mood/depression. My
clinical research has led me to understand that trauma, especially
complex-trauma, results in more than just disrupting brain/mind
functioning. This trauma gets imprinted
into the neurological circuitry of the brain and never goes away entirely. It
literally changes the ways in which the brain processes our experiences (figure 1). Leading me to the conclusion
that a lot more work is required in the healing process. I am not a big fan of
either cognitive-behavioral therapies or techniques done to a patient to
release them from their traumatic experiences. My neuro-psychoanalytic training
leads me in the direction of the interaction/interface of brain and mind as
being the most effective treatment for trauma.
And aren’t traumatic experiences the basis of all mental health
disorders.
Finally,
i am reminded that psychoanalytic treatment works by understanding that 1) the
unconscious runs all of us (figure 1). 2) the majority of our work in treatment is
helping patients resolve their resistances to creating their own health. 3) we are concerned with the patient’s
psychic structure. Exactly how are they processing their thoughts, feelings,
and actions, and those situations in the world around them. And exactly how all
this changes when the brain/mind is traumatized, especially over an extended
period of time. 4) neuro-psychanalysis adds the perspective that the human mind
is the subjective experience of the brain.
And this denotes the importance of the brain in our therapeutic work.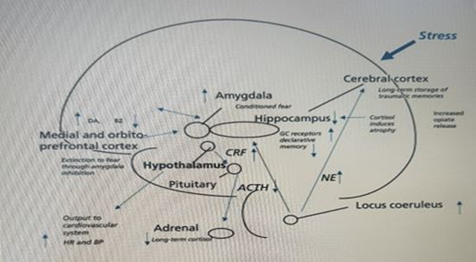
Figure 1: lasting effects of trauma on the brain, showing
long-term dysregulation of nonrephinephrine and cortisol systems and vulnerable
areas of hippocampus, amygdala and medial prefrontal cortex that are affected
by trauma. Gc, glucocorticoid; crf, corticotropin-releasing factor; acth,
adrenocorticotropin hormone; nf, norepinephrine; hr, heart rate; bp, blood
pressure; da, dopamine; bz, benzodiazapine; gc, glucocorticoid
In
part ii of this article, i will be exploring how “listening to the brain” helps
us free our patients from the prison of complex-ptsd.
References
1. Judith
h. Trauma and recover: the aftermath of violence-from domestic abuse to
political terror (revised edition), basic books, 2015.
2. How
ptsd and trauma affect your brain functioning,” psychology today posted on
2018.
3. how
ptsd affects the brain. Brainline. 2019.
4. bremner
jd. Traumatic stress: effects on the brain. Dialogues in clinical neuroscience
2006;8(4):445-461.
5. audrey
l, mckiernan e, prats-sedano ma, et al. Neuroimaging and clinical findings in
healthy middle-aged adults with mild tbi in the prevent dementia study. Jama
netw open 2024;7(8):e2426774.
6. aliev
g, beeraka nm, nikolenko vn. Neurophysiology and psychopathology underlying
ptsd and recent insights into the ptsd therapies: a comprehensive review. J
clin med 2020;9(9):2951.
7. maercker
a, cloitre m, bachem r, et al. Complex post-traumatic stress disorder. Lancet
2022;400(10245):60-72.
8. Hidden
effects of trauma and complex trauma in psychology posted, 2021.
9. Davis
s. Inflammation and the brain changes observed in c-ptst. Cptsd research, the
brain and cptsd, trauma informed. 2019.