An Unusual Case of Primary Parotid Tuberculosis Associated with Whartin’s Tumor: Case Report
Conclusion: the key lessons highlight the limited role of radiological imaging in the detection of parotid tuberculosis on one side and the crucial importance role of surgery, not only for confirming the diagnosis of tuberculosis but also for identifying associated tumors, which may be either malignant or benign on the other side.
Keywords: parotid tuberculosis; parotid cysadenolymphoma; whartin’s tumor; associated cystadenolympha; whartin’s tumor; parotid tuberculosis; extrapulmonary tuberculosis; salivary gland tuberculosis
Introduction
Parotid
tuberculosis is a rare form of extrapulmonary tuberculosis, even within endemic
countries like morocco. Clinical diagnosis can be very difficult and may lead
to misdiagnosis, as it resembles neoplasms during physical examinations and
imaging studies. In this study, we present a case of primary parotid
tuberculosis associated with a cyst adenolymphoma in a 66-year-old male patient
who underwent combined medical and surgical management. The patient's outcome
was very favorable, resulting in complete resolution of the disease.
Despite its infrequency, parotid tuberculosis generally has a positive prognosis if diagnosed and treated early. Surprisingly parotid gland tuberculosis has very rarely been reported in the literature especially in cases linked to warthin's tumor.
Case
report
A
66 years old male patient, without any particular medical antecedents. There was
no history of trauma or previous surgery or any contact with tb patient. The patient
was admitted in our department for a painless right parotid swelling increasing
in volume progressively, evolving since 6 months. Without limitation of the
mouth opening or peripheral facial paralysis or any other associated signs. All
evolving in a context of a good general state.
The
physical examination revealed a small painless and firm mass of the right
parotid region, mobile to the superficial and deep plan, measuring
approximatively 3 cm of grand axis, without any inflammatory signs in opposite.
The left parotid region is normal. The examination of the cervical lymph node
areas did not reveal any lymphadenopathy. The examination of the oral cavity
was normal, with no evidence of pus emission or inflammation in opposite. The rest
of the facial examination was unremarkable (figure 1).
Figure1: image showing the swelling of the right parotid region.
The cervical ultrasound performed showed a right parotid oval tumor lesion with regular contours, measuring 3 cm, most likely suggestive of a pleomorphic adenoma.
The facial mri showed a solid cystic oval formation, well
limited, seat of a multi-partitioned cystic component with heterogeneous
intermediate t2 signal and t1 hypersignal spread over 36 mm, with fine
peripheral contrast, describing an adc ratio of 0.94. The
right parotid and submandibular glands,
in addition to the thyroid are without signal or morphological abnormalities (figure
2).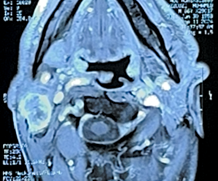
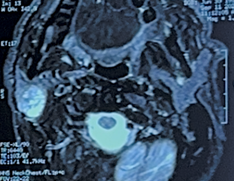
Figure
2: axial facial mri images showing: the
solid cystic formation in t1 and t2 signal.
The patient was discussed at a staff meeting and the decision was made to proceed with a surgical management. Therefore, the patient underwent a right superficial parotidectomy with an intraoperative frozen section, which revealed a right parotid tuberculosis.
The
definitive pathological examination revealed a warthin’s tumor, also known as
cyst adenolymphoma, completely excised and associated with evolving case
follicular tuberculosis, without any signs of malignancy.
The postoperative follow-up, after having benefited from a six-month course of antitubercular treatment, was very favorable. The patient did not experience any local recurrence and is in stable condition.
Discussion
Tuberculosis can affect any organ system in the body. Although
pulmonary tuberculosis is the most common form, extrapulmonary tuberculosis
(eptb) is also a significant clinical issue1,2.
It represents approximately 25% of overall tubercular morbidity3. This rarity is attributed to the
antibacterial properties of saliva and its continuous flow, which prevents the
accumulation of bacilli.
Among the various forms of extrapulmonary tuberculosis (eptb). Lymph node tuberculosis is the most prevalent type. Other types include skeletal, central nervous system, abdominal, genitourinary tuberculosis and tuberculous pericarditis4.
Parotid tuberculosis is a rare form of extra pulmonary tuberculosis. There are two primary theories regarding the pathogenesis of tubercular parotitis. The first theory proposes that the condition arises from the direct transmission of mycobacteria from an adjacent infected site in the oral cavity, such as the tonsils or teeth. This transmission may occur either through retrograde movement of the bacilli via the duct or through afferent lymphatic pathways. The second theory suggests that the infection could also spread to the gland through hematogenous or lymphatic transfer originating from the lungs5.
Clinically, parotid tuberculosis is generally presented as a unilateral swelling or abscess, involving the gland's parenchyma6. Late manifestations include pain, abscess formation, fistulas and facial nerve involvement. Although symptoms like cough, fever, weight loss and loss of appetite can occur with tuberculosis but they are relatively rare7,8.
Parotid tuberculosis is often mistaken for cancer or autoimmune diseases. Imaging tests typically lack specificity, making microbiological diagnosis essential for accurately identifying this condition9.
Radiological examinations, including ultrasound, ct and mri, are effective at identifying intraparotid tubercular lesions; however, the results often lack specificity and can resemble malignancies. Ct and mri are particularly useful for assessing the size of the lesion and identifying any deeper associated conditions. Due to the tumor-like appearance of the imaging results, many cases may necessitate surgical intervention, such as a superficial parotidectomy, with the diagnosis being confirmed postoperatively10. However, mri has a sensitivity of approximately 75% for detecting benign characteristics and this can be enhanced with contrast agents. Additionally, mri may offer a more accurate characterization of the disease compared to ct and ultrasound11.
Due to the non-specific nature of imaging findings, confirming a tuberculosis diagnosis necessitates histological evidence. Fine needle aspiration cytology (fnac) is highly sensitive and specific, making it the preferred initial approach for evaluating a parotid mass. However, their results can sometimes be inadequate or ambiguous. Such patients may be subjected to unwanted surgery10
The world health organization (who) recommends a six-month treatment regimen for drug-sensitive tuberculosis12.
This regimen consists of four drug regimen (rifampicin, isoniazid, ethambutol and pyrazinamide) in the intensive phase followed by two drugs (rifampicin and isoniazid) in continuation phase13.
Anti-tubercular medications should be initiated as soon as possible to ensure effective healing. While previous guidelines emphasized the importance of combining medical and surgical methods to prevent recurrence8. The current ones increasingly favors conservative management. When the surgical management is now primarily reserved for cases with residual enlargement of the parotid gland14,15.
Conclusion
The stenosis of the external auditory canal (eac) can be
congenital, due to abnormalities of the first gill cleft or acquired as a
result of inflammation, trauma and the effects of radiotherapy, all sharing a
common pathogenesis, namely a cascade of inflammatory changes leading to medial
canal fibrosis. The surgical aim is to produce a dry
and patent ear canal and also to improve hearing.
Management of acquired atresia requires a skin graft to cover the deficient ear canal, in addition to plug excision. However, the ear canal remains unstable and recurrence can occur.
References
1. Fanning
A. Tuberculosis: Extrapulmonary disease. CMAJ 1999;160(11):1597-1603.
2. Sharma
SK, Mohan A. Extrapulmonary tuberculosis Indian J Med Res 2004;120(4):316-353.
3.
Gopal R,
Padmavathy BK, Jayashree K. Extrapulmonary tuberculosis: A retrospective study
Indian J Tuberc 2001;49:225-6.
4. Farer
LS, Lowell AM, Meader MP. Extra pulmonary tuberculosis in USA. Am J Epidemiol
1992;109(2):205-217.
5. Cantrell
RW, Jensen JH, Reid D. Diagnosis and management of tuberculosis cervical
adenitis. Arch Otolaryngol 1975;101(1):53-57.
6. Garg
R, Verma SK, Mehra S, Srivastawa AN. Parotid tuberculosis. Lung India
2010;27:253-255.
7. Süoğlu
Y, Erdamar B, Cölhan I, Katircioğlu OS, Cevikbas U. Tuberculosis of the parotid
gland. J Laryngol Otol 1998;112(6):588-591.
8. Stanley
RB, Fernandez JA, Peppard SB. Cervical mycobacterial infections presenting as
major salivary gland disease. Laryngoscope 1983;93(10):1271-1275.
9.
Gupta N, Aggarwal A, Tripathi M, Nischal N.
Parotid
gland tuberculosis. QJM
2020;113:500-501.
10. Gupta
V, Patankar K, Shinde A, Bhosale C, Tamhane A. Tuberculosis of the parotid
gland. Case Rep Radiol 2012;2012:278793.
11. Iserì
M, Aydìner O, Celìk L, Peker O. Tuberculosis of the parotid gland. J Laryngol
Otol 2005;119:311-313
12. WHO
consolidated guidelines on tuberculosis, module 4: treatment - drug-susceptible
tuberculosis treatment.
13. World
Health Organization. Treatment of tuberculosis: Guidelines for national
programs WHO/CDS/TB/2003.313. 2003 Geneva WHO
14. Mastronikolis NS, Papadas TA, Marangos M, Karkoulias KP, Tsamandas
AC, Goumas PD. Tuberculosis of the parotid gland Tuberk Toraks 2009;57:84-88.
15. Chintamani,
Daniel R, Manu S, Bhushan V, Gupta K. Parotid TB. Trop Doct 2006;36(2) :119-120.