An Unusual Presentation of a Newly Diagnosed Right Colonic Adenocarcinoma Complicated with Right Lower Quadrant Colonic Abscess in an Elderly Man: A Case Report and Literature Review
ABSTRACT
Colorectal cancer is the third most common malignancy
and the second most lethal malignancy of the general population. Right sided
colon canceris less common than left sided, occurring more frequently in
females, and associated with an older age and poor prognosis. Intraabdominal
abscess formation is a rare complication from colorectal cancer. Thus, we
present a case of a 66-year-old male who presented to the emergency department
with 4 days of sudden onset, intractable right lower quadrant abdominal pain associated
with nausea and vomiting. After further evaluation, he was diagnosed with right
sided colon adenocarcinoma complicated by peri-colonic abscess formation. He
was treated with hemicolectomy without immunotherapy. Considering the scarcity
of data concerning colonic abscess formation and colorectal adenocarcinoma,
more research is needed on this dual presentation. These authors reinforce that
in older patients presenting with acute abdomen, colorectal cancer should be
noted as a differential.
Keywords: Colon
cancer; Colon abscess; Colon adenocarcinoma; Colon neoplasm; Colorectal tumor
INTRODUCTION
Colorectal cancer (CRC)is the third
most common cancer and the second leading cause of death in the USA. The
incidence rate is 140,000 cases/year and the mortality rate is 55,000
cases/year1,2. Typical presenting
symptoms related to colorectal cancer include a change in bowel habits with
increasing constipation or spurious diarrhea, lower abdominal pain, decreased
stool caliber, visible blood in the stool, weakness, and weight loss. Carcinoma
of the colon has theability to mimic any abdominal disease with a wide spectrum
of presentations. For example, some less usual manifestations include perforation
and abscess formation, which are usually intraperitoneal but may also be
located in the extraperitoneal spaces3. Right sided
colon cancer occurs predominantly in females of older age groups. Additionally,
it is less common than left sided colon cancer, with anemia occurring more
frequently, associated with poor outcome at the later stage of the disease4. Colon cancer complicated with
abscess formation is rare with occurrence of about 0.3–4% of the cases andcan
occur due to colon perforation, fistula formation or tumor extension5. Hence, we present an unusual case of a
66-year-old man who was diagnosed with right sided colon cancer complicated
with peri-colonic abscess and was treated with antibiotics and hemicolectomy
without immunotherapy. Since there is still little data about the occurrence of
abscesses in colon cancer patients, more research is needed. In addition, colon
cancer should be considered as a differential in older individuals presenting
with acute abdomen.
CASE PRESENTATION
A 66-year-old male presented to the
emergency department with 4 days of sudden-onset, intractable right lower
quadrant pain associated with nausea and vomiting. Laboratory values were
significant for leukocytosis of 12 cells/mm3 (reference 4-11.2), hyponatremia
of 129 mmol/L (reference 136-145), and acute kidney injury with blood urea
nitrogen (BUN) 38 mg/dL (reference 7-18) and creatinine 1.52mg/dL (reference
0.7-1.3). Vitals were stable on admission. Past medical history was significant
for Schizophrenia for which he claimed compliance with oral ziprasidone 100mg
twice daily. Initial imaging with CT abdomen/pelvis
without contrast demonstrated narrowing of the ascending colon, possibly due to
the presence of a mass. Surrounding layering free fluid with a few small foci
of air within a collection measuring approximately 5.1 x 10.8 x 16.3 was
demonstrated, as seen in (Figure 1)
below.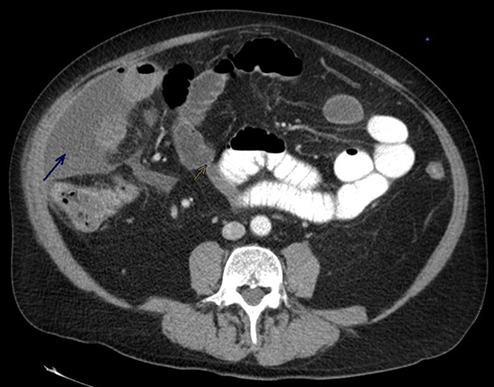
Figure 1. Computed Tomography of
Abdomen with contrast. Blue Arrow pointing to layering free fluid foci with
apical pockets of air surrounding the ascending colon and yellow arrow pointing
to the stricture caused by the cancer.
A repeat CT
abdomen/pelvis with oral and IV contrast was performed the same day to further
characterize the mass, and this demonstrated an enlarging fluid and air
collection of approximately 11.9 x 4.4 x 16.1 within the lateral right abdomen,
suggestive of an abscess. Notably, an irregular appearance of the cecum with
possible luminal breaks suggesting perforation was also observed. A fistulogram
was later performed which confirmed leaking into the peritoneum. The patient
also had increased opacities within the lung bases, suggestive of atelectasis
and/or pneumonia.
Of note, the patient had
a colonoscopy performed 3 years prior to the current presentation, which
pathology defined as a tubular adenoma with high grade dysplasia in the sigmoid
colon and a hyperplastic rectal polyp. Both lesions were removed in their entirety
via snare polypectomy with electrocautery and excisional biopsy, respectively.
A diagnosis of a peri
colonic abscess complicated by cecal perforation (with fecal peritonitis) was
made, and CT guided aspiration + insertion of a 12F locking pigtail catheter
into the right lower quadrant abscess was performed. The catheter drained
purulent fluid and samples yielded cultures positive for Bacteroides
fragilis, Escherichia coli and Propionibacterium granulosum.
The patient continued the Metronidazole 500mg IV q8h that was started on
admission and was switched from empiric piperacillin/tazobactam to Meropenem 1g
IV q8h, as well as started on Doxycycline 100mg IV q12h to target the Propionibacterium
granulosum. While the patient remained afebrile and the leukocytosis,
hyponatremia and renal impairment resolved throughout admission, he did have
diarrhea on days 3-5 of admission, prompting testing for Clostridium
dificile, which resulted negative. Abdominal XRAY confirmed multiple loops
of dilated small bowel, which subsequently resolved, and the diarrhea resolved
with the use of Loperamide.
Differential diagnoses
for cecal abscess were explored, and a cecal mass or perforated appendicitis
were considered. However, in view of the low yield and high risk for
colonoscopy in the acute inpatient setting, the colonoscopy was deferred to the
outpatient setting. As the fistula became low output, the Jackson-Pratt drain
was continuedand the patient was started on oral diet, and switched to oral
antibiotics (Levofloxacin 750mg daily, Metronidazole 500mg q8h and Doxycycline
100mg q12h for 21 days total). The colonoscopy was performed shortly after
discharge. Colonoscopy revealed moderately differentiated adenocarcinoma of the
right colon and distal ileum without lymphovascular and/or perineural invasion,
placing the tumor at stage IIA (pT3N0). The patient then proceeded to have a
right hemicolectomy with subsequent reversal of the ileostomy. He wasfollowed
by the hematology/oncology department where he was managed by sequential
monitoring without chemotherapy given that the tumor was totally removed.
DISCUSSION
As a result of various risk factors
and associated comorbidities, colorectal cancer is one of the most frequently
diagnosed malignancies in the western world. It continues to be the third most
common malignancy and the second most lethal malignancy of the general
population6. Its lethality can be
attributed to its various presentations observed in patients. The frequently
associated presentation of colon cancer is early satiety, change in bowel
habits, stool caliber, occult blood in stool, accompanied by common malignancy
presentation: Weight loss, lymphadenopathy, anemia, and fatigue. However, there
are several reports of colorectal cancer that have deviated from this
presentation and have made the action of early diagnosis difficult. One such
presentation is the formation of an abscess with adjuvant growing CRC. The
incidence of abscess formation in relation to CRC is 0.3-4% of CRC cases making
it an unusual presentation4,7. Abscess
formation can be within the colonic tract, as in our patient, or extra-colonic
tract. There have been reports of primary presentation of pyogenic liver
abscess, peri-rectal abscess, abdominal wall abscess or in severe cases abscess
with fistula presentation with a secondary CRC diagnosed later in the hospital
or disease course. Due to the variety of locations
where abscess can be formed in the abdominal cavity and reports of CRC
diagnosis being associated with several abscess locations, it is difficult to
pinpoint an exact abscess location. However, due to increasing reports of abscess
formation, signs of an abscess in the abdominal tract, can mask a silent CRC. Due
to the poor prognosis of CRC with disease progression, early detection of CRC
is crucial to the management and treatment of these patients and for their
future lifestyles. There have been limited studies on the treatment of CRC with
associated abscess formation due to the rarity of the presentation, and
therefore, treatment regimens have not been completely investigated on the
efficacy of treating the CRC and the abscess. However, patients who present
with signs of infection or findings of abscess formation, investigation of
underlying CRC should be a priority, as early detection can be used to gain
time to treat the cancer and achieve a good prognosis for the patient.
In past literature CRC have been
associated with several different bacteria. Strong association of C.septicum
and S. Bovis infective endocarditis exist with colon cancer. However,
this does not mean that all abscess are associated with the former bacteria. As
in our case to which cultures tested negative, other bacteria could be
causative for abscess formation. Other bacteria that have been isolated include
anerobic bacteria. CRC growth in the colon results in disruption of the mucosal
barrier stripping the defense protection of the colon and disrupting the flora
leading to the entrance of several bacteria into the gastrointestinal and
systemic circulation8, with subsequent bacterial colonization
in the abdominal cavity organs exposed8 demonstrated
that tumor cells can spread transcoelomic and disseminate, which led to
future disseminated recurrences and poorer prognosis after primary treatment6. A common
presentation of CRC is to spread into the surrounding structure and organs
leading to its obstructive symptoms. However, obstruction can lead into
perforation into the adjacent structures leading to the abscess formation.
Right sided colon cancers is more common among females and presents with signs of
anemia which is contrary to our patient who was a male and came with symptoms
of obstruction4. clinically classified three proposed
mechanisms to subsequent complications after perforation by CRC: 1) Perforation
into the peritoneal cavity 2) covered perforation with local abscess formation;
3) perforation into one of the neighboring organs7. Abscess
formation can happen simultaneously with CRC growth as evidenced by a
73-year-old man who presented with malignancy symptoms and in imaging
circumferential ulcerated type tumor in the lower to upper right rectal wall
was shown with a 23 × 22 mm perirectal abscess on the ventral side of the
rectum that had invasion into the bladder7. In this
case, the patient presented with malignancy symptoms rather than infectious
symptoms. However, the opposite can occur as demonstrated by8, who
reports a 77-year-old man who presented appendicitis, laparotomy, excision of
the appendicular abscess located between the ascending colon and the
retroperitoneum was done. Cultures of the abscess fluid yielded Proteus
vulgaris, Prevotella bivia, and Flavo bacterium species seen in the abdominal
cavity. Pathological specimen from that surgery revealed differentiated cecal
adenocarcinoma staged 3B. 6 months later the patient came again for liver
metastases. This presentation is seen in 25-30% of elderly patients who present
with appendicitis8. Another case is of a 50-year-old woman
diagnosed primarily with abscess in the Douglas pouch and ovarian cancer,
however, subsequent workup revealed 5.5-cm-diameter round mass was located
adjacent to the sigmoid colon in the pelvic cavity and was diagnosed with an abscess
and sigmoid colon cancer8. In a case analysis by9, 61
patients with 98% having a diagnosis of CRC were studied9. The study
identified 87.2% of patients had an iliopsoas muscle abscess, and CT imaging
did not detect simultaneous tumors. The study demonstrated right colon
adenocarcinoma as a strong association for retroperitoneal abscess8. Lastly,
another case is of a 32-year-old woman with an initial diagnosis of
gastroenteritis with a presentation of LLQ pain10. Lack of improvement led to imaging identifying
an abscess which was promptly treated, however, continued to recur. This led to
a colonoscopy which displayed a stricture. Pathology confirmed invasive
adenocarcinoma. Culture of the abscess identified B. Fragilis- anerobic
bacteria that normally colonizes the colon10 identified B.Fragilis
in purulent pericarditis that eventually led to a diagnosis of CRC11. The
conclusion of these cases reveal that CRC associated abscess formation does not
have limitations in the causative bacterial agents, location, age or type of
CRC. Therefore, diagnosing CRC with a primary presentation of infectious
etiology becomes difficult. However, due to increasing incidence of this rare
presentation, CRC should become a differential diagnosis when presented with a
patient who does not improve with treatment of abscess or continues to have
recurrent abscesses as there could be an underlying sinister CRC causing
obstruction and perforation.
The treatment of
abscess associated with CRC is not a fixed regimen, due to the rarity of the
presentation. Treatment in these cases often occurs due to the later stages of
CRC growth and invasion. As described above, abscess is often formed after
perforation of the tumor into colon and adjacent structures. In addition,
patients present with symptoms and laboratory markers for infectious etiology
from the abscess. Therefore, treatment is primarily for the abscess. The
misdiagnosis allowing the tumor to continue to grow, invade, and perforate. Most
cases in literature have described it difficult to differentiate between the
tumor mass and the abscess and subsequently identifying a resection line as complicated.
There has been a discussion on whether the abscess should be treated first,
with incision and drainage, so that the primary disease can be clear and then
be treated or that both the abscess and the tumor mass be resected
concurrently. However, the latter raises argument for seeding of tumor or the
abscess during operation and further spreading of the cancer and patient
tolerance for a large surgery. Successful treatment entails early surgical
treatment as described by8. Supportively, reported surgical
mortality and 5-year survival rates of 50 % and 20 %, respectively, in patients
with colon cancer complicated by local abscess8. In most of
the cases included in this article, due to the high risk of micro metastases
and poor condition and prognosis of the patient it was noted that abscess
treatment was primarily executed. In addition, there is no correlation between
the extent of abscess and survival and prognosis of the cancer. Prognosis of
the cancer is dependent on the staging and tumor invasion. Therefore, it can be
concluded that no illustrated benefit of resection of cancer and abscess
together. Abscess treatment included antibiotics, incision and drainage, or
excision, in particular with intra-colonic location and subsequent colostomy. However,
comment to the former, if the colonic location is more proximal and in the
ascending colon, resection is advised. After treatment of abscess, early
surgical treatment with neoadjuvant chemotherapy is advised for resection of
the tumor to prevent perforation or metastases7.
CONCLUSION
Colorectal cancer
continues to be a malignancy that is very much prevalent in the general
population. It was commonly thought to be a cancer that was seen in the
geriatric population, however, due to new screening guidelines CRC is seen in
younger populations. Although there are commonly associated symptoms and signs
that are attributed to CRC, there have been reports of rare comorbidities and
associations. One such presentation is an abscess formation with an underlying
CRC. Although, there have been very limited studies to study this association
due to its rarity, it should be considered a differential in patients who are
poorly responsive to infectious treatments or who continue to have recurrent
abscesses. Definitive diagnosis is most frequently obtained by surgical
resection and specimen confirmation by pathology. In our patient, hemicolectomy
was done with no further treatment. Therefore, due to the scanty data on
colonic abscess and colorectal cancer, more research is needed. These authors
advocate early management and highlight that in older persons with acute
abdomen, underlying colorectal cancer should be considered as a differential.
Declaration
Funding: Not applicable
Conflict of interest/Competing
interests: All participating
authors declared no conflict of interest.
Ethics Approval: Not applicable
Consent to Participate: Not applicable.
Written consent for publication: We hereby give the consent for our paper to be published under the
traditional submission.
Availability of Data: Our data and materials will be available for research and learning
purposes. The Data used to support the findings of this study are included
within the manuscript.
Code availability: not applicable.
Author’s contribution: Divine
Be song AA, Palmer Victoria, Annmarie Theresa
participated in the conception of the work, writing and supervision. Derek
Ugwendum, Sefakor Akosua Atadja, Nancelle Ndema, Nkafu B,Kankeu T,contributed to literature search. Sabastain Forsah,
Ababio Agyemang., Zafar Wahib,Foma Kenne Munoh , Jay
Nfonoyim was involved in data acquisitionwriting and
supervision. All authors read and approved the final manuscript.
REFERENCES
2. Mann GN, Scoggins CR, Adkins B. Perforated cecal
adenocarcinoma presenting as a thigh abscess. South Med J 1997;90(9):949-951.
3. Mármol I, Sanchez-de-Diego
C, Dieste AP, Cerrada E, Yoldi MJR. Colorectal Carcinoma: A general overview
and future perspectives in colorectal cancer. Int J Mol Sci 2017;18(1):197.
4. Bustamante-Lopez LA, Nahas SC, Nahas CSR,
Pinto RA, Marques CFS, Cecconello I. Is there a difference between right
-versus left -sided colon cancers? does side make any difference in long-term
follow-up? Arq Bras Cir Dig 2019;32(4):1479.
5. ElGendy
K, Al Duhileb M, Salem A. Transverse colon cancer presenting as acute abdominal
wall abscess. BMJ Case Rep
2014;2014.
6. Menon G, Recio-Boiles A, Lotfollahzadeh S,
Cagir B. Colon Cancer. StatPearls 2023.
7. Yano T, Nakano K,
Yoshimitsu M, Idani H, Okajima M. Successful resection of rectal cancer and
perirectal abscess following systemic chemotherapy and chemoradiotherapy: A
case report. Int J Sur Case Rep
2023;108:108403.
8. Atsushi O, Kubo Y, Tanada M, Kurita A,
Takashima S. Unusual abscesses associated with colon cancer: Report of three
cases. Acta Medica Okayama
2007;61(2):107-113.
9. Zhou J, Wan S, Li C,
et al. Retroperitoneal abscess as a presentation of colon cancer: The largest
case set analysis to date, which extracted from our unit and the literature. Front Oncol 2023;13:1198592.
10. Hiroyuki S, Kidder
I, Tanaka T, Goto M. Incidence of colorectal cancer in patients diagnosed with
pyogenic liver abscess. JAMA Network
Open 2023;6(12):2348218.
11. Harbison JA. Colon
Cancer Masquerading as Recurrent Abdominal Abscesses. J Case Rep Images Oncology 2019;5(1):1.