Atypical Herpes Zoster Oticus: Case Report and Review of Literature
ABSTRACT
Introduction and Importance: Herpes zoster oticus, or Ramsay Hunt syndrome,
is a rare neurological pathology caused by the varicella-zoster virus
reactivating in the facial nerve's geniculate ganglion. Its importance lies in
the description of a rare case of cranial nerve palsies.
Case presentation: A 19-year-old previously healthy man was
admitted to our emergency department complaining of an intense right otalgia in
the last two days, without improvement with simple analgesia. Symptoms were
complicated by right facial palsy, mild proper hearing loss, dysgeusia, and
vertigo 24 hours later. On physical examination, he was alert and
oriented, with a Glasgow score of 15/15, without focal neurologic deficit
except for right-sided peripheral facial palsy: Grad V of House–Brackmann
scale. On otoscopy, he had no visible vesicular eruption nor any abnormalities.
Clinical discussion: Sicard syndrome, also known as Herpes
zoster oticus or Ramsay Hunt syndrome, is a rare neurological condition caused
by the reactivation of latent VZV in the geniculate ganglion of the 7th cranial
nerve.
Clinical diagnosis is mainly
based on interrogation findings and clinical examination. Three clinical
pictures are possible:
1. The diagnosis is usually easy when the
vesicular rash occurs before or simultaneously with the facial palsy
2. Yet, sometimes, the rash develops only after
the onset of facial palsy
3. And finally, a minority of patients, like our
case, do not develop any vesicular lesions at all.
Conclusion: Early diagnosis and adequate treatment by
virostatic agents and corticosteroids are crucial to improve damaged nerves and
maximize and hasten the chances of full recovery.
Keywords: Herpes zoster oticus; Sicard syndrome; Lagophthalmo;
Ipsilateral palsy
INTRODUCTION
Ramsay Hunt syndrome or herpes zoster oticus due to
varicella-zoster virus infection is commonly reported in immunocompromised
individuals or patients aged at least 50. It is responsible for 16% of
unilateral facial paralysis in children and 18% in adults. Its classic triad is
composed of vesicle-cracked lesions in the concha, ipsilateral palsy, and
lagophthalmos.
In fact, immunosuppression, advanced age, pregnancy,
lack of vaccination against the varicella-zoster virus, and physical and
psychological stress are major factors that predispose to the reactivation of
the virus, which may invade the central nervous system. Diagnosis is based on a
bundle of arguments: clinical history and physical examination. Further
investigations, such as an MRI, can be carried out to rule out differential
diagnoses.
We report a case of Ramsay Hunt syndrome in a young
man without any underlying pathology. This highlights the importance of early
diagnosis to minimize neurological damage and emphasize that even if the
clinical triad appears late or is incomplete, treatment must be early for a
significant improvement in symptoms and quality of life.
This
work has been reported as being in line with the SCARE criteria.
CASE PRESENTATION
A 19-year-old previously healthy man was admitted to
our emergency department complaining of an intense right otalgia in the last
two days, without improvement with simple analgesia. Symptoms were complicated
by right facial palsy, mild proper hearing loss, dysgeusia and vertigo 24 hours
later. He denied fever, tinnitus, hyperacusis, nausea or vomiting. On physical
examination, he was alert and oriented, with a Glasgow score of 15/15, without
focal neurologic deficit except for right-sided peripheral facial palsy: Grad V
of House-Brackmann scale. On otoscopy, he had no visible vesicular eruption nor
any abnormalities (Figures 1 and 2).
Figure 1: Right-sided facial palsy grade 5 according to House-
Brackmann facial grading scale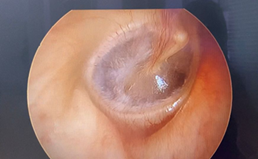
Figure 2: Normal tympanic membrane
He also had gait ataxia and was complaining of
rotatory vertigo, all of which made vestibular examination difficult. However,
he had no dysmetria on finger-to-nose and heel-to-knee tests.
With the clinical findings, the diagnostic hypothesis
of Herpes zoster oticus was suggested.
During hospitalization, further investigations were performed. Brain MRI
showed an asymmetric enhancement in the right facial nerve after contrast
administration, suggesting right facial neuritis (Figure 3).
Pure tone audiometry examination revealed increased
bone and air conduction thresholds in frequency ranges approximating 1000 Hz
and exceeding 2000 Hz on the right side, suggesting sensorineural hearing
loss.
Vestibular tests showed decreased VOR gains of the
right anterior and lateral semicircular canals (Figure 4). Videonystagmography revealed a homogeneous pursuit and
a left preponderance. In contrast, in the caloric testing, a right areflexia
with a deficit of 93% was obtained (Figures
5,6,7).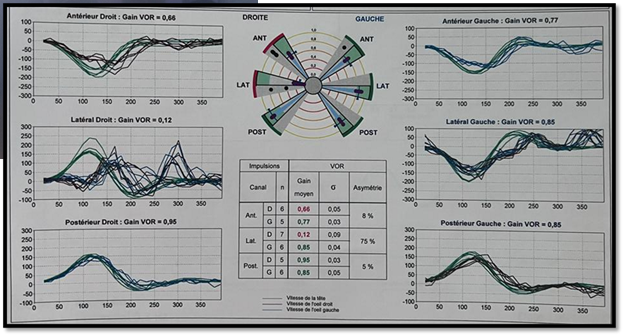
Figure 3: A video head
impulse test of the patient before the treatment shows decreased VOR gains of
the right anterior and lateral SCC.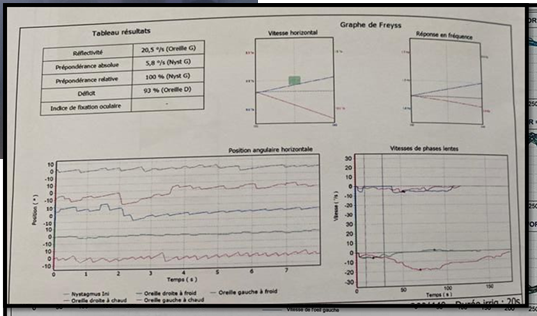
Figure 4: Caloric testing reveals right
areflexia in low frequencies that have not yet been compensated, with a
significant left preponderance.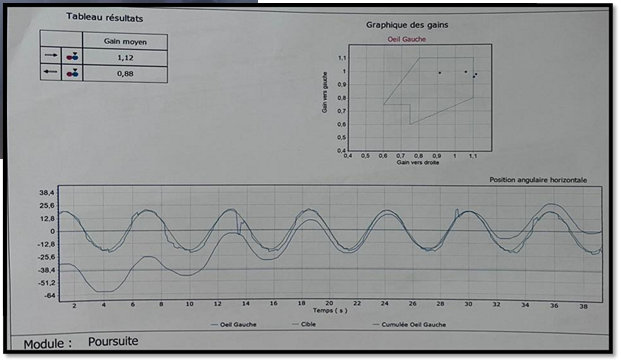
Figure 5:
Smooth pursuit testing with no abnormalities.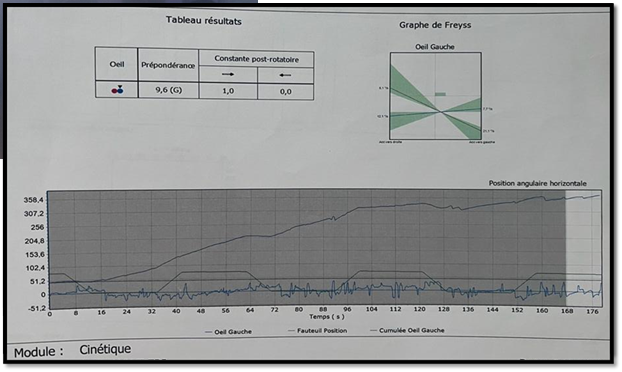
Figure 6:
This test shows an important left preponderance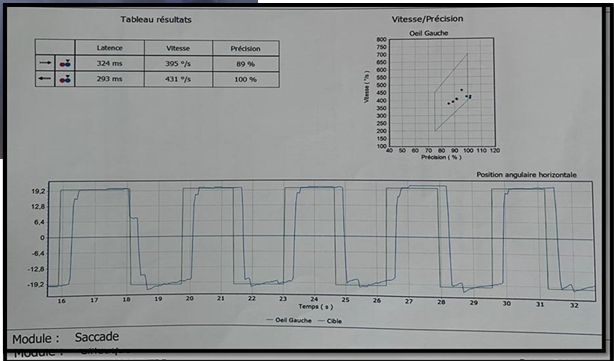
Figure 7:
No saccadic disorder detected in Videonystagmography tests
Medication included intravenous acyclovir 10 mg per kg
every 8 hours for 14 days and prednisolone 1mg/kg for five days. Physiotherapy
for the face and facial nerve rehabilitation was initiated, as well as vitamin
B therapy, proper eye protection, and humidifying eye drops. Vestibular
rehabilitation was also initiated during the hospitalization.
The patient slowly improved and showed complete
improvement in gait. After four days, he was discharged from the hospital to
complete home treatment and return to follow-ups. He had a grade III of the
House Brackmann Facial Nerve scale system at discharge (Figure 8).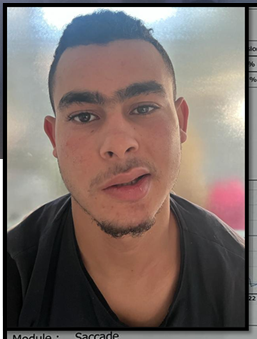
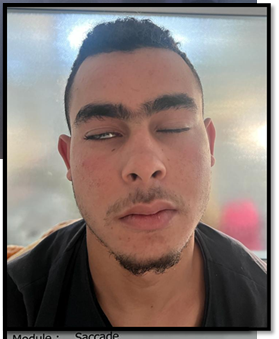
(A) (B)
Figure
8: Improvement of facial function after four
days of intravenous treatment.
After one month, he presented partial improvement in the facial palsy. He is in grade II of the House Brackmann Facial Nerve scale system.
No vertigo, no gait ataxia was found. Control
vestibular testing showed a VOR gain of the right lateral SCC of 0.30 vs. 0.12
and a VOR gain of the right anterior of 0.93 vs. 0.66.
At caloric testing, we noted a well-compensated right
hypo valence and a reflective lateral SCC on both the right and left (Figures
9,10). 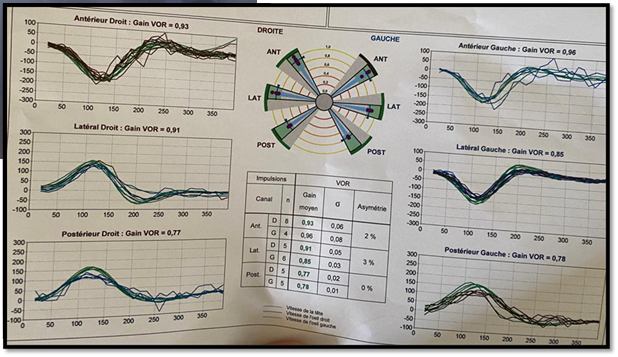
Figure 9: Video head impulse test
after one month, showing normal VOR gains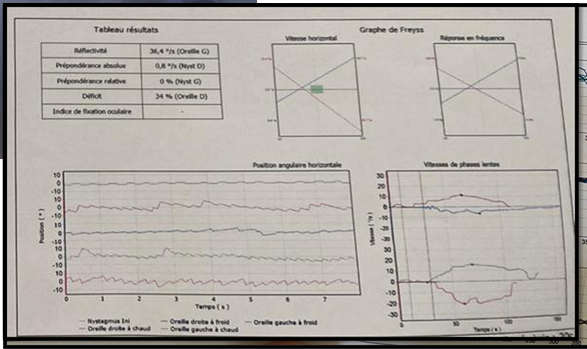
Figure 10:
Control caloric testing after one month
DISCUSSION
Facial nerve paralysis is idiopathic in more than 70%
of cases (Bell’s palsy). However, other varied pathologies can be responsible
for acute facial nerve paralysis: autoimmune diseases, sarcoidosis,
neurological diseases, temporal bone trauma, iatrogenesis, neoplasms (glomus
tumor, vestibular schwannoma, parotid), as well as Varicella-zoster virus, and
cytomegalovirus infections1.
icard syndrome, also known as Herpes zoster oticus or
Ramsay Hunt syndrome, is a rare neurological condition due to the reactivation
of latent VZV in the geniculate ganglion of the 7th cranial nerve2.
The RHS was first described in 1906, and many case
reports and clinical and pathologic studies have been published. However, the more is published, the less this
syndrome is understood. Either because of its rarity or because of the
unpredictable clinical condition3,4.
Hunt established a classification of his syndrome in
four different clinical groups5:
2. Herpes oticus with facial
palsy.
3. Herpes oticus with facial
palsy and auditory symptoms.
4. Herpes oticus with facial
palsy with accompanying auditory and labyrinthine symptoms.
This classification was based on the hypothesis that
the pathologic process of this disease is taking place at the geniculate
ganglion. Yet, since the publication of this classification, many authors have
questioned the validity of the geniculate ganglion theory between 1907 and
1967. Consequently, the consistent finding in autopsies was a widespread
lymphocytic infiltration along the entire facial nerve, not just about the
geniculate ganglion6,7.
The incidence of zoster oticus appears less in
children who receive the varicella vaccine than in children who contract
varicella infection, suggesting that vaccination might prevent herpes zoster
infection and prevent or reduce the occurrence of Ramsay Hunt syndrome.
However, the reactivation of latent varicella zona virus is triggered by a
decrease in patient cell-mediated immunity8.
Clinical diagnosis is mainly based on interrogation
findings and clinical examination. In fact, regarding the timing of the
vesicular rash and the facial palsy, three clinical pictures are possible9:
2. Yet,
sometimes, the rash develops only after the onset of facial palsy,
3. And
finally, a minority of patients, like our case, do not develop any vesicular
lesions at all.
Although the triad blister pustule crusted lesions in
the external ear around the Ramsay Hunt region, lagophthalmos, and finally,
peripheral ipsilateral facial paralysis are sufficient to make the RHS
diagnosis10; However, clinical
diagnosis can sometimes be difficult when faced with a polymorphic and
dissociated presentation11.
Other symptoms may occur, such as hearing loss,
tinnitus, dizziness, and, less frequently, dysgeusia, nasal obstruction, dry
eye, and dysarthria12.
In the case described here, attention is drawn to the
lack of dermatological lesions. Further tests may be performed to rule out
other possible differential diagnoses. Virological and serological diagnoses
are particularly interesting in the face of severe and atypical forms.
Polymerase chain reaction assays may be useful to detect herpes zoster virus
DNA in exudates from ear lesions or cerebrospinal fluid13. In addition, brain MRI can visualize
inflammation of the cranial nerves14.
Regarding treating herpes zoster oticus, intravenous
administration of virostatic agents such as acyclovir in combination with
corticosteroids is highly recommended. It should be administered early to
improve acute pain and reduce the duration of active disease, reducing neural
damage and preventing postherpetic neuralgia.
The virostatic agent acyclovir is recommended at a
dose of 10 mg/kg in adults and 500 mg/m2 in children every 8 hours for a
minimum duration of 7 to 10 days, followed by oral treatment of 7 days.
Corticosteroid therapy is controversial; the dose is generally 1 mg/kg/day in
10 days, has potent anti-inflammatory action, and is well tolerated15.
However, it seems that there is no difference between
the use of oral versus intravenous antiviral agents16. What matters is starting treatment in the first 48 hours
of clinical symptoms, as we did in this case, which is a crucial prognosis
factor in preventing nerve damage17.
Treatment also involves adequate analgesia and motor
physiotherapy to treat motor sequelae,
which tend to be more severe and less likely to improve when compared to Bell's
palsy18.
CONCLUSION
Ramsay Hunt syndrome is defined by zoster oticus,
which involves the seventh and the eighth cranial nerves. It is characterized
by acute facial palsy and vestibulocochlear dysfunction with a herpetic
eruption on the auricula and external ear. Polymorphous and dissociated
clinical presentations are possible, which shows the diagnosis challenges of
this syndrome, especially in the absence of a typical vesicular rash.
Early diagnosis and adequate treatment by virostatic
agents and corticosteroids; is crucial to improve damaged nerves and maximize
and hasten the chances of full recovery. This allows us to conclude that the
prognosis depends on the timing at which the combined therapy is started.
The patient provided written informed consent for the
publication of this case report and accompanying images. The editor-in-chief of
this journal can review a copy of the written consent upon request.
Ethics statement: Ethics
approval is not needed in case reports in our institution's research structure.
Conflict of Interest: All authors have no
potential conflicts of interest to disclose.
REFERENCES
1. Tankere
F, Bernat I. Paralysie faciale a frigore : de l’étiologie virale à la réalité
diagnostique. Rev Medecine Interne 2009;30(9):769‑775.
2. Rouihi
A, Errami N, Hemmaoui B, Benariba F. Zona otitique, aspects cliniques et therapeutiques
: a propos d’un cas. Pan Afr Med J 2022;41:171.
3. Devriese
P. XC Facial Paralysis in Cephalic Herpes Zoster. Ann Otol Rhinol Laryngol 1968;77(6):1101‑1119.
4. Payten
RJ, Dawes JD. Herpes zoster of the head and neck. J Laryngol Otol 1972;86(10):1031‑1055.
5. Sachs
Jr E, House RK. The Ramsay Hunt Syndrome, Geniculate herpes. Neurology 1956;6(4):262‑262.
6. Aviel
A, G. Marshak, Ramsay hunt syndrome: A cranial polyneuropathy. Am J Otolaryngol
1982;3(1): 61‑66.
7. Guldberg-Møller
J, Olsen S, Kettel K. Histopathology of the facial nerve in herpes zoster
oticus. JAMA Arch Otolaryngol 1959;69(3):266‑275.
8. Kansu
L, Yilmaz I. Herpes zoster oticus (Ramsay Hunt syndrome) in children: Case
report and literature review. Int J Pediatr Otorhinolaryngol 2012;76(6):772‑776.
9. Kanerva
M, Jones S, Pitkaranta A. Ramsay Hunt syndrome: characteristics and patient
self-assessed long-term facial palsy outcome. Eur Arch Otorhinolaryngol 2020;277(4):1235‑1245.
10. Gondivkar
S, Parikh V, Parikh R. Herpes zoster oticus: A rare clinical entity. Contemp
Clin Dent 2010;1(2):127‑129.
11. Sauvaget
E, Herman P. Zona auriculaire. EMC Oto Rhino Laryngol 2012;7(4):240‑245.
12. Monsanto
R, Bittencourt A, Bobato NN, Beilke S, Lorenzetti F, Salomone R. Treatment and prognosis
of facial palsy on ramsay hunt syndrome: Results based on a review of the
literature. Int Arch Otorhinolaryngol 2016;20(4):394‑400.
13. Sauerbrei
A, Eichhorn U, Schacke M, Wutzler P. Laboratory diagnosis of herpes zoster. J
Clin Virol 1999;14(1):31‑36.
14. do
Amaral LB, Ferro CA, Guerra LC, et al. Ramsay hunt syndrome: a case report.
MedNEXT J Med Health Sci 2023;4(3).
15. Wagner
G, Klinge H, Sachse MM. Ramsay Hunt syndrome. JDDG 2012;10(12):238-243.
16. Murakami
S, Hato N, Horiuchi J, Honda N, Gyo K, Yanagihara N. Treatment of Ramsay Hunt
syndrome with acyclovir‐prednisone: significance of early diagnosis and
treatment. Ann Neurol 1997;41(3):353‑357.
17. Rocha
A, Leal F, Martins MD, Mendes M, Silva B, Nogueira L. Ramsay-Hunt syndrome : A
case report. Authorea 2023.
18. Sohrabi
C, Mathew G, Maria N, Kerwan A, Franchi T, Agha RA. The SCARE 2023 guideline: Updating
consensus Surgical Case Report (SCARE) guidelines. Int J Surg Lond Engl
2023;109(5):1136.