Atypical Presentation of an Anomalous Right Coronary Artery
Abstract
Anomalous right coronary
artery is a rare congenital disorder, which is usually asymptomatic and
diagnosed incidentally. Symptoms usually manifest in the young adulthood and
show a wide range of manifestations, including sudden cardiac death. The
symptoms are mainly exertional because of the intramural course of anomalous
coronary, making it vulnerable to compression during activity. We report a case
of a patient with anomalous right coronary artery presenting atypically at an
older age with angina occurring even at rest. This case was diagnosed on a
coronary angiography and treated successfully with coronary unroofing.
Keywords:
Cardiology; Internal medicine; Anomalous coronary arteries
INTRODUCTION
Anomalous
origin of the right coronary artery arising from the left coronary sinus and
taking an interarterial course between the great vessels is a rare diagnosis,
with a reported incidence between 0.026% and 0.250%1. With most cases being asymptomatic, the anomalous right
coronary artery is typically diagnosed incidentally on cardiac imaging2. However, cases can also present with sudden
cardiac death, when they are found to have anomalous coronaries during autopsy.
Most of the symptomatic cases have been reported to occur before the age of 35
with exertional angina, and some even presenting with sudden cardiac death3. We report a case with this rare diagnosis
that presented atypically with angina, occurring even at rest, and had a late
presentation at an older age.
CASE PRESENTATION
A
46-year-old female presented with a year-long history of intermittent episodes
of retrosternal chest pain, radiating to the jaw, neck and the left arm. These
episodes occurred both during the activity and at rest. They were severe enough
to disrupt her sleep and worsened progressively over time, leading to multiple
office and emergency department visits for the patient. Electrocardiogram
showed normal sinus rhythm without any ST segment changes, and troponins were
normal. Lexiscan stress test revealed normal myocardial perfusion with no
obvious ischemia and no transient ischemic dilatation (TID). Echocardiogram
revealed normal ejection fraction of 55-60% without any regional wall motion
abnormalities. Left heart catheterization showed normal left main coronary
artery, left anterior descending and left circumflex artery, however, the RCA
could not be engaged. Eventually, coronary CT angiogram was done which showed
an anomalous right coronary artery originating from the left coronary cusp with
an intramural course, with reformatted images revealing compression of the
proximal RCA between the proximal pulmonary artery and the aorta (Figures 1 and 2). The patient had
already failed medical management by the time this diagnosis was made, as she
had been tried on different drugs including antianginals, non-steroidal
anti-inflammatory drugs across her multiple office visits.
Figure 1.
Coronary CT angiogram showing anomalous origin of the right coronary artery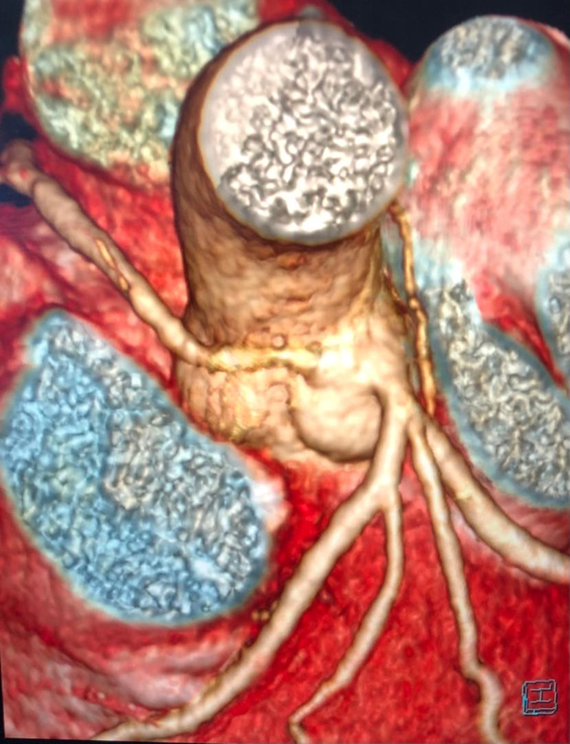
Figure 2.
Coronary CT angiogram showing anomalous origin of the right coronary artery (3D
image)
Patient
was then referred to cardiothoracic surgery. She got coronary unroofing of the
abnormal origin of the anomalous origin of the right coronary artery. Her
intraoperative course was complicated by severe biventricular dysfunction on
the first attempt off cardiopulmonary bypass (CPB) which resolved on the second
attempt. Post operative course was unremarkable and she was discharged on post
operative day four. At one and three month follow up visits, patient reported
marked improvement and resolution of her symptoms.
DISCUSSION
Anomalous
origin of a coronary artery (AAOCA) can be defined as the origin of coronary
artery occurring at or above the incorrect sinus of Valsalva (Figure 3). These are further
classified based on the course they take as inter-arterial, subpulmonic,
pre-pulmonic, retroaortic, or retrocardiac. Although both them are very rare in
incidence, anomalous inter-arterial RCA has higher reported incidence (six
times more) than the anomalous inter-arterial LCA4.
Inter-arterial coronaries, between the aorta and pulmonary artery, typically
take an early intramural course between the intimal and adventitial layers of
the aortic root5. Our case had
anomalous origin of right coronary artery originating from the left coronary
cusp, taking an interaterial course with an intramural segment.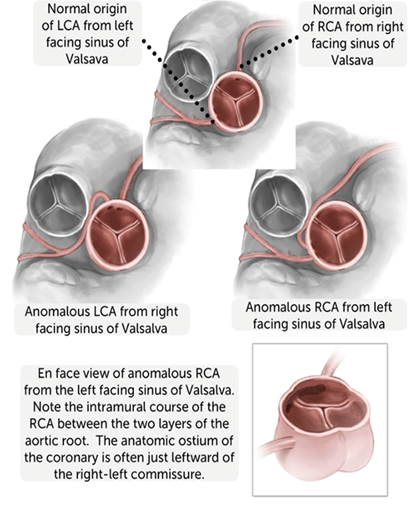
Figure 3.
Description of normal and anomalous coronary artery origin
Most
of these cases are asymptomatic and only diagnosed incidentally. When
symptomatic, anomalous RCA typically manifests before the age of 35 as ischemic
symptoms during exertion3. Two
mechanisms have been proposed. One, the elongated and narrow anomalous RCA is
unable to provide enough perfusion due to the increased myocardial oxygen
demand during exercise, creating a demand supply mismatch. Second, aorta
dilates during exertion, which causes compression of the anomalous RCA against
the pulmonary artery. The sharp angulation and slit like ostium of the
anomalous RCA further makes it vulnerable to compression during aortic
dilation.
Our
case had an atypical presentation as the patient presented late for this
congenital disorder with symptoms starting in late fourth decade. Furthermore,
patient had angina occurring even at rest, rather than just during exertion.
This case points that congenitally anomalous RCA should remain as a
differential for the elderly or mid age presentation for angina. Angina at rest
may be an indicator of a precarious coronary anatomy in our case. Given the
paucity of evidence and difficult measurement techniques, there are no clear
guidelines stratifying the risk for anomalous RCA based upon the anatomy like
length of intramural segment, degree of angulation etc. Further studies are
needed to determine this risk. Coronary imaging through CT angiogram or MRA is
not only the best test to diagnose this condition, but can also help in
determining the key anatomical features of the anomalous coronary artery. These
imaging features, along with the clinical presentation and shared decision
making can play a role in determining the appropriate cases for definitive
surgical intervention.
Different
surgical techniques have been used for repair of anomalous coronaries, with
coronary unroofing being the most commonly used technique2 (Figure
4). Other surgeries include coronary reimplantation, CABG, patch
augmentation or combination of these. Coronary unroofing used in our case,
involves opening up the intramural course of the anomalous coronary, to
effectively create a new orifice in the correct sinus of Valsalva6 (Figure
4). in their larges study of 148 patients undergoing coronary unroofing,
showed excellent early outcomes with no intraoperative and post operative
mortality and 94% late survival rates7. 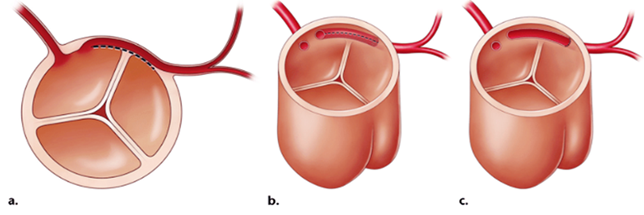
Figure 4.
Diagram showing technique of coronary unroofing for an interaterial coronary
with an intramural segment. The intramural course is opened up over its entire
length (along the dashed line in a & b), thereby creating a wide neo-ostium
without angulation or a slit like opening (c).
CONCLUSION
Anomalous
RCA may present at an elderly age, atypically with angina occurring even at
rest. Concrete understanding of the wide symptomatology of this rare disorder
will help make physicians make early diagnosis and intervention to prevent
malignant arrythmias and sudden cardiac death among these patients. Coronary
unroofing is the definitive treatment, which has shown excellent intra and post
operative outcomes.
Grant
Funding: None/Not Applicable
REFERENCES
1. Greet
B, Quinones A, Srichai M, Bangalore S, Roswell RO. Anomalous right coronary
artery and sudden cardiac death. Circ Arrhythm Electrophysiol
2012;5(6):e111-e112.
2. Penalver JM, Mosca RS, Weitz D, Phoon CK. Anomalous aortic
origin of coronary arteries from the opposite sinus: a critical appraisal of
risk. BMC Cardiovasc Disord 2012;12:83.
3. Basso C, Maron BJ, Corrado D, Thiene G. Clinical profile of
congenital coronary artery anomalies with origin from the wrong aortic sinus
leading to sudden death in young competitive athletes. J Am Coll Cardiol
2000;35(6):1493-1501.
4. Swaminath D, Panikkath R, Strefling J, Rosales A, Narayanan
R, Wischmeyer J. Anomalous Right Coronary Artery from Left Main Coronary Artery
and Subsequent Coursing between Aorta and Pulmonary Trunk. Case Rep Med
2013;2013:195026.
5. Lee BY. Anomalous right coronary artery from the left
coronary sinus with an interarterial course: Is it really dangerous? Korean
Circ J 2009;39(5):175-179.