Bilateral Slipped Capital Femoral Epiphysis - A Rare Presentation of Primary Hypothyroidism
Abstract
Primary hypothyroidism, characterized by
insufficient thyroid hormone production, has other systemic effects with SCFE
being unrecognized and a rare presentation. This case report aims to present a
rare occurrence of bilateral SCFE in the context of primary hypothyroidism. We
present the case of a 19-year-old boy who initially presented with symptoms of
bilateral hip pain and limited mobility. Diagnostic evaluation revealed
concurrent primary hypothyroidism, confirmed through thyroid function tests.
Subsequent imaging confirmed the presence of bilateral slipped capital femoral
epiphysis. The patient received appropriate thyroid hormone replacement and is
planned for surgical intervention for SCFE. This case highlights the importance
of considering underlying endocrine disorders, such as primary hypothyroidism,
in the differential diagnosis of atypical presentations of SCFE. Further
research is needed to understand the exact pathophysiological mechanisms by
which primary hypothyroidism causes bilateral SCFE.
Keywords: Slipped capital femoral
epiphysis; Primary hypothyroidism
While primary hypothyroidism is known to affect multiple organ systems, its association with SCFE is relatively uncommon and has not been extensively reported in the literature.
This case report aims to present a rare occurrence of primary hypothyroidism presenting as bilateral SCFE. We highlight the importance of considering underlying endocrine disorders in the differential diagnosis of atypical presentations of SCFE.
Understanding this association may provide insights into the pathophysiology and optimal management of both primary hypothyroidism and SCFE.
Case Report
A
19-year-old boy who was born out of nonconsanguineous marriage through a normal
vaginal delivery at term with an uneventful prenatal and postnatal period with
normal developmental milestones presented with non-traumatic limping and
bilateral hip pain which worsened over the last 6 months.
There
was a history of weight gain (7 kg in the last 6 months), constipation,
fatigue, dry skin and increased sleepiness.
No
significant family history was noted.
On Examination
Physical
examination revealed short stature (height: 156 cm; mid-parental height: 177.5
cm) with a BMI of 22.5 kg/m². Clinical findings included dry, coarse skin,
facial puffiness, periorbital swelling, a diffuse smooth goiter and delayed
relaxation of deep tendon reflexes. Bilateral testicular volume was normal (25
cc), with a stretched penile length of 9 cm.
Laboratory investigations showed markedly elevated TSH levels (772 mIU/mL), with low T4 and T3 concentrations. Prolactin, cortisol, testosterone levels and calcium profile were within normal limits. Bone age assessment showed delayed skeletal maturity and pelvic imaging (x-ray pelvis) confirmed bilateral slipped capital femoral epiphysis (SCFE) (Table 1).
The
patient was diagnosed with primary hypothyroidism and initiated on
levothyroxine supplementation at 50 mcg/day. He is scheduled for corrective
osteotomy to address SCFE (Figure 1).
Table
1: Biochemical
Investigations
|
Parameter |
Values |
Reference range |
|
|
|
TSH |
772 mIU/ml |
0.5-5 mIu /ml |
|
|
|
FREE T4 |
<0.88 mcg/dl |
5.2-11 mcg/dl |
|
|
|
PROLACTIN |
27.4 ng/ml |
<20 ng/ml |
|
|
|
8AM CORTISOL |
6 mcg/dl |
(5-15 mcg/dl ) |
|
|
|
ACTH |
21.2 mcg/dl |
>18 mcg/dl |
|
|
|
STIMULATED CORTISOL |
|
|||
|
TOTAL TESTOSTERONE |
281.3 ng/dl |
200-970 ng/dl |
|
|
|
LH |
0.996 mIU/ml |
0.8-8.7 miu/ml |
|
|
|
FSH |
8.96 mIU/ml |
1.2-9.6 IU/L |
|
|
|
CALCIUM |
9.3mg/dl |
Calcium-8.5-10.5 mg/dl |
|
|
|
PHOSPHOROUS |
4.2 mg/dl |
Phosphorous-2.5-4.5 |
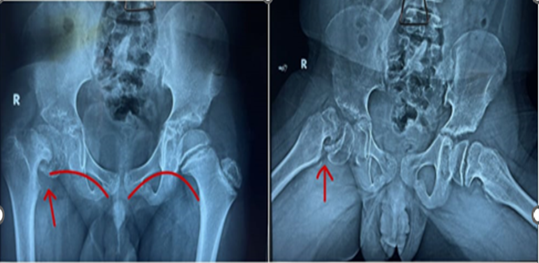
Figure 1: The Antero-Posterior and Frog Leg Lateral Radiograph of Pelvis with Both Hips Showing Evidence of Severe Chronic Stable Scfe On The Right Hip With A Pre &Post Slip On The Left Hip. It Also Shows Evidence Of Open Triradiate, Capital Physis, Greater Trochanter In Both The Hips-Which Is Unusual In A 19 Year Old.
Treatment
He was initiated on levothyroxine therapy (50
mcg/day) and is being planned for corrective osteotomy to address the bilateral
slipped capital femoral epiphysis (SCFE).
Discussion
Slipped
Capital femoral epiphysis (SCFE) is a rare disorder with a prevalence of 10.8
cases per 100,000 children2,4. It
primarily affects the adolescent age group. However, adults can be affected if
epiphyseal closure is delayed because of an underlying endocrine disorder like
hypothyroidism.
Hypothyroidism
is an endocrine condition marked by insufficient production of thyroid
hormones, which play a crucial role in normal growth, development and bone
metabolism1. Thyroid hormone
deficiency in children results in delayed endochondral and intramembranous
ossification, as well as hypoplasia of the epiphyseal plate (growth plate).
Additionally, it impairs the growth hormone/insulin-like growth factor axis.
Recent studies in animals, including hypothyroid swine, have shown a notable
reduction in the expression of proteoglycans and type X collagen in the growth
plate5.
In
hypothyroidism, impaired chondrocyte function can delay growth plate closure
and increase the risk of SCFE.
Furthermore,
primary hypothyroidism often coexists with other endocrine disorders, such as
growth hormone deficiency or hypopituitarism, which could also contribute to
the development of SCFE6,7. Loder et
al. studied 85 individuals with SCFE associated with endocrine disorders and
reported that 40% were diagnosed with hypothyroidism, 25% with growth hormone
deficiency and 35% with other conditions, including panhypopituitarism and
hyperparathyroidism8. In our patient,
a comprehensive hormonal workup to rule out other hormonal causes showed no
abnormalities.
Management of primary hypothyroidism presenting with bilateral SCFE requires a holistic approach. Treatment focuses on optimizing thyroid hormone levels through hormone replacement. Surgical intervention is frequently required to stabilize the femoral head and prevent further slippage.
This case report emphasizes the importance of thyroid function screening in patients with SCFE, particularly those presenting in adulthood, with short stature or bilateral involvement.
More case reports will help elucidate the pathophysiology and potential risk factors for SCFE in individuals with primary hypothyroidism.
Conclusion
SCFE should be considered in adults with
bilateral hip pain and limping, with a focus on evaluating for endocrine
associations, particularly primary hypothyroidism, which is a treatable
condition.
SCFE is a preventable disorder in these
patients if diagnosed early.
Conflicts of Interests
Nil
Funding
None
References
2. Lehmann CL, Arons RR,
Loder RT, Vitale MG. The epidemiology of slipped capital femoral epiphysis: an
update. J Pediatr Orthop 2006;26:286-290.
3. Novais
EN, Millis MB. Slipped Capital Femoral Epiphysis: Prevalence, Pathogenesis and
Natural History. Clin Orthop Relat Res 2012;470(12):3432-3438.
4. Gholve PA, Cameron DB,
Millis MB. Slipped capital femoral epiphysis update. Curr Opin Pediatr
2009;21(1):39-45.
5. Yen PM. Physiological and
molecular basis of thyroid hormone action. Physiol Rev 2001;81:1097-1142.
6.
Boyce AM, Shawker TH, Hill SC,
et al. Bilateral slipped capital femoral epiphysis: Hormonal and metabolic
factors. J Bone Miner Res 2013;28(3):516-526.
7.
Brambani F, Bianchini G,
Todescan R. Bilateral slipped capital femoral epiphysis and primary
hypothyroidism. J Pediatr Orthop 1988;8(1):101-103.
8. Loder RT, Wittenberg B,
DeSilva G. Slipped capital femoral epiphysis associated with endocrine
disorder. J Pediatr Orthop 1995;15:349-356