Comparative Analysis of CT Outcomes in COVID-19: Non-Vaccinated Individuals vs. Vaccine Breakthrough Cases
ABSTRACT
Background: In the context of the COVID-19 pandemic, this study investigates
the influence of vaccination on patient demographics and clinical outcomes.
Exploring disparities aids in refining public health strategies.
Purpose: To investigate and compare demographics, comorbidities, and
clinical characteristics between vaccinated and unvaccinated COVID-19 patients.
Methods: This prospective observational study conducted between January
2021 and June 2022, evaluates CT outcomes in COVID-19 patients relative to
vaccination status. Data collection encompasses demographics, comorbidities,
and clinical details. Two radiologists independently use a CT Severity Score
(CTSS) to evaluate pneumonia extent, exploring associations with age, gender,
and vaccination status through statistical analyses.
Results: Out of 1020 patients, 220 were excluded. The study analysed data
from 800 patients, with 450 vaccinated and 350 unvaccinated. Demographics and
comorbidities showed no significant differences between groups. Dyspnoea and
sore throat were more frequent in the unvaccinated group (p < 0.05).
C-reactive protein levels were consistently elevated in both groups (>80%),
indicative of COVID-19 (p > 0.05). These data provide a comprehensive
overview of the patient population, highlighting differences in demographics,
comorbidities, and clinical characteristics between vaccinated and unvaccinated
individuals. There were no noticeable differences in frequency between patients
who had received vaccinations and those who had not.
Conclusions: Vaccination status showed no significant correlation with
comorbidity, symptom severity, or clinical outcomes. Younger individuals and
females, regardless of vaccination status, showed less lung involvement. Lower
CT severity scores associated with vaccination emphasize its significance in
adults, guiding future COVID-19 research and strategies.
Keywords: COVID-19; Computed tomography; Demographic characteristics;
Vaccination; CT severity score; Vaccine breakthrough cases
INTRODUCTION
The year 2019 marked the onset of a global crisis that
transcended borders, reshaped societies, and challenged the resilience of
healthcare systems worldwide the COVID-19 pandemic. Caused by the novel
coronavirus SARS-CoV-2, this viral outbreak swiftly evolved from a localized
health concern to a complex, multifaceted global emergency1. In the
wake of the unprecedented global health crisis sparked by the COVID-19
pandemic, the scientific community has witnessed an extraordinary convergence
of efforts aimed at developing effective vaccines against the novel
coronavirus, SARS-CoV-222. Vaccination campaigns, pivotal in mitigating the impact of the
virus, have faced both acclaim for their role in reducing severe illness and
criticism amid the emergence of breakthrough infections in vaccinated
individuals3,4.
Although
mild to severe sickness can be brought on by breakthrough coronavirus
infections, in vaccinated and unvaccinated population. However, the likelihood
of a major COVID-19 infection is extremely rare, particularly in those without
a chronic illness5,6. Tan et al
(2023)7 found that another
coronavirus strain, omicron, more infectious than the one taken into
consideration during vaccine development, caused breakthrough infection in 28%
population compared to 36% of unvaccinated people. They also estimated that the risk of transmitting
infection was reduced by 22%, 23%, and 40% among vaccinated breakthrough,
infected prior and both vaccinated and infected priorly respectively7.
Vaccines, a pandemic beacon, raise questions on real-world
efficacy, especially with emerging variants and waning immunity. CT outcomes in
COVID-19 guide diagnosis, treatment decisions, research, public health
strategies and understanding the long-term impact of the disease on the
respiratory system8,9. This study unravelled the impact of infections in
non-vaccinated individuals and breakthrough infections among the vaccinated-on
CT outcome of patients. We also compared the nuances of vaccine effectiveness on
individuals from different demographic backgrounds.
MATERIAL AND METHODS
Study Design and Population
It was a prospective observational study conducted from Jan
2021-Jun 2022. The study enrolled 1020 patients who came for the CT scan at our
hospital. Patients who agreed to be part of the study and filled patient
information sheet and informed consent form were included in the study.
Patients who were not interested in study and/ or had a history of severe
respiratory diseases were excluded from the study. Finally 800 Patients were
included in the study.
Among 1020 patients, we identified 450 individuals who had
received both doses of the any recommended COVID 19 vaccine between Jan 2021
and Jun 2022 and who had a documented positive SARS-CoV-2 PCR based on nasopharyngeal swab testing within 7 days of registration to our centre. These
people are recognized as having breakthrough infections. We also identified 350
Individuals from the unvaccinated control group tested positive for COVID19
infection within last 14 days.
Data collection
Informed consent form and general questionnaire related to
demographic data were collected from each patient. By reviewing each case demographic,
laboratory, co-morbidity and clinical data were collected. The population was
divided based on age and sex (Demographic characteristics) and comorbidities
(cardiovascular disease, diabetes, hypertension, and cancer) and clinical
symptoms (cough, fever, sputum, myalgia, sore throat, and sensory loss).
Each patient's CT images taken during hospitalization were
retrieved from the department. It was obtained within a week of symptom onset.
CT scan
Interpretation
Unaware of the patient's clinical details, two radiologists
(Senior and Junior) examined every image and results were compared in
consensus. Person who is under training (resident) was considered as junior
radiologist, whereas a radiologist with over 20 years of experience in thoracic
imaging was considered as senior radiologist. Analysis was done on the amount
of pneumonia on the CT scans taken within a week of onset of symptoms. Based on
research predicting the severity of COVID-19 the amount of pneumonia in all
five lung zones on CT scans was graded as CT Severity Score (CTSS). It ranged
from 0 to 5 (score 0: no evidence of pneumonia, score 1: 1%–5% involvement,
score 2: 5–25% involvement; score 3: 26–50% involvement; score 4: 51–75%
involvement; score 5: > 75% involvement. Total score of all lobes ranged
from 0 to 2510. A typical appearance was thought to be multifocal round
ground-glass opacities (GGOs) or peripheral bilateral GGOs, with or without
intralobular lines, consolidation, or a reverse halo sign. The definition of an
uncertain appearance was having GGOs, either with or without consolidation, but
without characteristic traits. The absence of typical or ambiguous
characteristics along with distinct centrilobular nodules, lung cavitation,
smooth interlobular septal thickening with pleural effusion, and/or lobar
and/or segmental consolidation without GGOs were considered uncommon
appearances11.
Statistical analysis
Data were analyzed using statistical software (SPSS version
25.0, IBM Corp). Continuous variables were expressed as median value and
interquartile range (IQR). The frequencies of demographic and clinical
characteristics of populations were expressed as the number (percentage) of
occurrences and were compared using the 2-tailed χ2 test. For the CTSS
assessment, the intraclass correlation coefficient (ICC) was used to compute
the interobserver agreement between the two radiologists. Univariate logistic
regression was performed to identify relationships between the CTSS and
independent variables (age, gender, and vaccination status) and for the outcome
analysis. Differences for which p < 0.05 were considered statistically
significant.
RESULTS
Comparative study of Demographic and
clinical characteristics based on the vaccination status
A
total of 1020 patients were enrolled for the present study. Among them, 220
were excluded from the study because they were either not interested in the
study or had severe respiratory illness (Figure 1). Demographic,
clinical, and laboratory data was collected for a total of 800 patients, who
were included in the study. Patients were majorly categorized into vaccinated
(n=450) and unvaccinated (n=350) groups. Among the total patients, 412 were males, and 388 were females with
median age 58). Gender distribution indicates that an equal proportion
of vaccinated and unvaccinated individuals are male and females (Ratio 1:1).
The age is reported as a median with an interquartile range (IQR), showing
comparable ages between the vaccinated (60 [42, 74]) and unvaccinated (56 [44,
71]) groups. The study highlights higher prevalence of hypertension and
diabetes in unvaccinated COVID-19 patients. Vaccinated individuals exhibit more
frequent fever and cough, while dyspnea and sore throat are more common in the
unvaccinated group. Elevated C-reactive protein levels, over 80% in both
groups, are identified as a consistent COVID-19 marker. (Table 1). The data offer a comprehensive
overview, revealing distinctions in demographics, comorbidities, and clinical
traits between vaccinated and unvaccinated individuals, with no significant
frequency differences.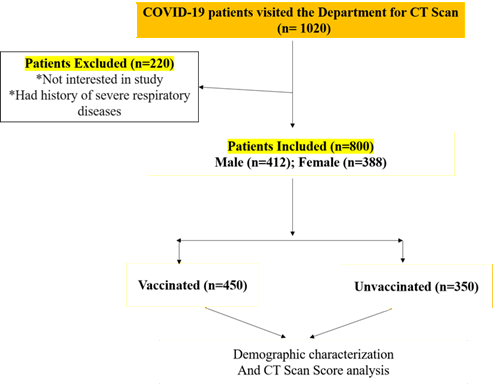
Figure 1. Flow chart of study methodology
Table
1. Comparative
analysis of demographic, clinical, and laboratory findings of vaccinated and
unvaccinated population
|
Variable |
All patients (n = 800) |
Vaccinated (n = 450) |
Unvaccinated (n = 350) |
|
Gender |
|||
|
Male |
412 (51.5%) |
231 (51.3%) |
181 (51.7%) |
|
Female |
388 (48.5%) |
219 (48.7%) |
169 (48.3%) |
|
Age * |
58 [40, 74] |
60 [42, 74] |
56 [44, 71] |
|
Comorbidities |
|||
|
No comorbidities |
280 (35%) |
149 (33.1%) |
131 (37.4%) |
|
Cardiovascular disease |
95 (11.9%) |
50 (11.1%) |
45 (12.8%) |
|
Diabetes |
159 (19.5%) |
70 (15.5%) |
86 (24.5%) |
|
Hypertension |
180 (22.5%) |
85 (18.9%) |
95 (27.1%) |
|
Cancer |
10 (1.25%) |
7 (1.5%) |
3 (0.9%) |
|
Others |
79 (9.8%) |
39 (8.7%) |
40 (11.4%) |
|
Symptoms |
|||
|
Fever |
612 (76.5%) |
383 (85.1%) |
229 (65.4%) |
|
Cough |
576 (72%) |
365 (81.1%) |
211 (60.3%) |
|
Dyspnea |
310 (38.8%) |
151 (33.6%) |
159 (45.4%) |
|
Sore throat |
710 (88.75%) |
380 (84.44%) |
330 (94.28%) |
|
Sensory loss |
90 (11.25%) |
50 (12.5%) |
40 (10%) |
|
Clinical and laboratory findings |
|||
|
Leukopenia |
102 (12.8%) |
67 (14.9%) |
35 (10%) |
|
CRP level |
696 (87%) |
387 (86%) |
309 (88.3%) |
|
PaO2/FiO2 ratio |
273 (34.1%) |
152 (33.8%) |
121 (34.6%) |
Table
2. Univariate
analysis based on CTS score
|
Variable |
CTSS (Junior Radiologist) |
CTSS (Senior Radiologist) |
|
Vaccination
status (all patients) |
||
|
Unvaccinated |
9
[3, 21] |
10
[2, 22] |
|
Vaccinated |
3
[0, 20] |
3
[0, 20] |
|
p |
< 0.001 |
< 0.001 |
|
Vaccination
status (only patients with CTSS > 0) |
||
|
Unvaccinated |
13
[8, 19] |
13
[9, 18] |
|
Vaccinated |
7
[4, 14] |
8
[3, 14] |
|
p |
< 0.001 |
< 0.001 |
|
Gender |
||
|
Male |
8
[0, 22] |
8
[0, 23] |
|
Female |
5
[0, 22] |
5
[0, 21] |
|
p |
< 0.001 |
< 0.001 |
|
Age |
||
|
41-58 |
7
[0, 19] |
8
[1, 19] |
|
59-75 |
10
[0, 23] |
11
[0, 22] |
|
P |
< 0.001 |
< 0.001 |
Assessment of CT severity score (CTSS) according to Vaccination Status
There
was good agreement between junior and senior radiologists in the interobserver
variability analysis (ICC of 0.89) for the CTSS assessment. The median time
interval between symptom onset and CT scan was 6 days4,7 for
vaccinated and unvaccinated patients (p = 0.312). (Tables 2) represent
the specified findings as reported by both junior and senior radiologists.
According to the senior radiologist, the CTSS results of all patients showed a
significant difference between vaccinated and unvaccinated patients
(p < 0.001), with a median value of 3 [0, 20] for vaccinated patients and 10
[2, 22] for unvaccinated patients. A similar statistical difference between the
two groups was confirmed (p < 0.001) when patients without lung involvement
(CTSS = 0) were excluded. The median CTSS was 8 and 13 for vaccinated and
unvaccinated individuals (Table 2). Males showed a higher median value (8) compared with females
(5). When parenchymal involvement was compared based on age, senior citizens
were noted with significantly (p < 0.001) higher median CTS scores compared
to adults (Table 2).
According
to both radiologists, GGO was the most common pattern in both vaccinated and
unvaccinated individuals, followed by crazy-paving and consolidation; among
vaccinated patients, GGO and crazy-paving patterns were more common (p <
0.001). Regarding the existence of pleural effusion and swollen lymph nodes,
there were no differences between individuals who had received vaccinations and
those who had not.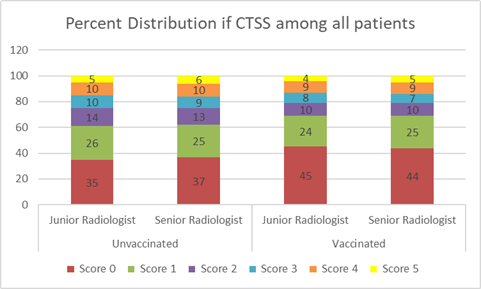
Figure
2. CT scan
scores of all unvaccinated and vaccinated patients involved in the study Assessment of the Proportions of Chest CT Scores Overall,
of the 800 patients included in the study, 480 patients (60%) underwent chest
CT during hospitalization; of these, 37% of unvaccinated patients and 45% of
fully vaccinated patients had negative CT scans (CTS Score 0). The proportion
of negative CT scans was higher in the fully vaccinated group than in the
unvaccinated group (p < 0.005) (Figure 2). Approximately 25% of
unvaccinated and vaccinated patients had a CT score of 1. Additionally, 13% of
unvaccinated patients and 10% of vaccinated patients had a CT score of 2. The
number of cases was not significantly different for CT scores 3, 4, and 5 (Figure
2).
Results
of vaccinated and unvaccinated patients having CTSS more than zero were also in
agreement between both radiologists. The severity of the disease was low in the
case of vaccinated people. Significantly a greater number of cases were
distributed for scores 1 and 2 for vaccinated patients. There was a significant difference in
frequencies of patients with higher CTSS 3, 4, and 5. It was 15, 16, and 11 for
unvaccinated and 12, 9, and 6 for vaccinated patients respectively (Figure
3).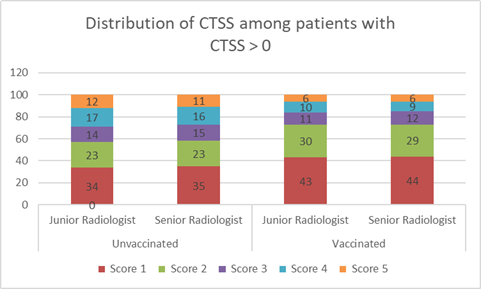
Figure
3. Distribution
of unvaccinated and vaccinated patients having CT scan scores more than 1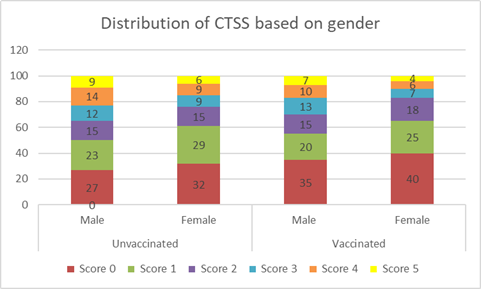
Figure
4. Distribution
of CT scan scores of all unvaccinated and vaccinated patients based on gender
We
noted that vaccination was effective in controlling lung damage for both males
and females. However, a greater number of females were unaffected (CTS score 0)
than males in vaccinated and unvaccinated groups. The severity of COVID-19
(scores 4 and 5) in females was less in vaccinated group (6,4) compared to the
unvaccinated group (9, 6 respectively). A similar trend was observed in males
as well (Figure 4).
Comparing
the age groups and vaccination statuses, it appears that there are variations
in the distribution frequency of both group for CTS scores. However, in both
age ranges, a higher number of vaccinated individuals have lower CTS scores
compared to the unvaccinated group. This trend is also observable in the 59-75
age group. On comparing scores on each group, comparatively higher number of
patients were distributed towards scores 1 and 2 for 41-58 years and 3,4 and 5
for 59-75 years (Figure 5).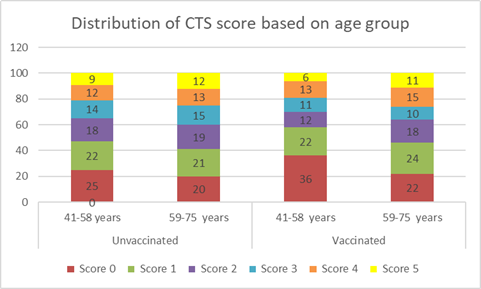
Figure
5. Distribution
of CT scan scores of all unvaccinated and vaccinated patients based on age
groups
DISCUSSION
The
investigation focused on the comparison of CT scan scores among vaccinated and
unvaccinated patients based on multiple factors such as age, sex, co-morbidity,
and symptoms. The CT scan was scored from 0-5 based on the severity of lung
involvement10. The findings of this
study indicate that vaccination status had no significant correlation with the
presence of co-morbidity, the severity of symptoms, and clinical outcomes in
COVID-19 patients.
Interestingly,
lower lung involvement was noted in younger people and females, irrespective of
their vaccination status. This analysis supported the recent findings,
demonstrating Chest CT features of COVID-19 patients11, however12 did not found any co relation among
COVID-19 symptoms with age, sex. This could be due to the inherent
immune responses across different age groups and genders12. According to13
men are more susceptible than women because they produce more testosterone
(TLT). Women's immune systems are stronger and can fend off severe SARS-CoV-2
viral disease because they express more of the TLR7 gene, which is located on
the X chromosome and encodes Toll-like proteins. This means that women's
dendritic cells can produce more interferons and antiviral proteins13. However, a deeper exploration into the
underlying causes of this observation is needed to develop a comprehensive
understanding of the disease progression in different demographic groups.
The
study observed a potential link between vaccination and lower CT scores,
indicating potentially milder lung involvement in COVID-19-infected vaccinated
individuals, aligning with prior imaging studies10,11,14,15.
It
underscores the importance of vaccination in adults for potentially reducing
the severity of the disease. Although further studies are required to establish
a definitive correlation, these findings provide preliminary evidence
supporting the role of vaccination in disease management.
The
lack of association between vaccination status and the presence of
co-morbidity, severity of symptoms, and clinical outcomes might seem
intriguing. It could be inferred that vaccination may not directly influence
these factors, but have a role in controlling the extent of lung damage, as
indicated by lower CT scan scores. However, many studies noted a significant
correlation of Co-morbidities and clinical outcomes with CT severity score16,17.
CONCLUSIONS
Vaccination
status had no association with the presence of co-morbidity, the severity of
symptoms, and clinical outcomes of COVID-19 patients. Lesser lung involvement
was noted for younger people and females irrespective of vaccination
status. A potential association between
vaccination and lower CT scan scores was noted, which highlights the importance
of vaccination in adults. These findings could be instrumental in shaping
future research and strategies for COVID-19 treatment and prevention.
Acknowledgements:
none
Conflicts
of Interest: nil
Funding:
None
REFERENCES
1.
Ciotti
M, Ciccozzi M, Terrinoni A, Jiang WC, Wang CB, Bernardini S. The COVID-19
pandemic. Crit Rev Clin Lab Sci 2020;57(6):365-388.
2.
Ciotti
M, Ciccozzi M, Pieri M, Bernardini S. The COVID-19 pandemic: viral variants and
vaccine efficacy. Crit Rev Clin Lab Sci 2022;59(1):66-75.
3.
Le
TT, Cramer JP, Chen R, Mayhew S. Evolution of the COVID-19 vaccine development
landscape. Nat Rev Drug Discov 2020;19(10):667-668.
4.
Bok
K, Sitar S, Graham BS, Mascola JR. Accelerated COVID-19 vaccine development:
milestones, lessons, and prospects. Immunity 2021;54(8):1636-1651.
5.
Lang
R, Humes E, Coburn SB, et al. Analysis of severe illness after postvaccination
COVID-19 breakthrough among adults with and without HIV in the US. JAMA Netw
Open 2022;5(10):2236397.
6.
Butt
AA, Yan P, Shaikh OS, Mayr FB, Omer SB. Rate and risk factors for
severe/critical disease among fully vaccinated persons with breakthrough severe
acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection in a high-risk
national population. Clin Infect Dis 2022;75(1):849-56.
7.
Tan
RY, Wong B, Lim R, Lee CL, Tan J, Tan KB, Wee LE. Factors associated with
delayed diagnosis of symptomatic adult COVID-19 cases presenting to primary
care: A population-wide study during transition from Delta to Omicron BA. 1 in
Singapore. Lancet Reg Health-West Pac 2023;41.
8.
Crombé
A, Bensid L, Seux M, et al. Impact of Vaccination and the Omicron Variant on
COVID-19–related Chest CT Findings: A Multicenter Study. Radiology
2023;307(3):222730.
9.
Lee
JE, Hwang M, Kim YH, et al. Imaging and clinical features of COVID-19
breakthrough infections: A multicenter study. Radiology. 2022;303(3):682-692.
10.
Lee
JE, Hwang M, Kim Y-H, et al. Imaging and clinical features of COVID-19
breakthrough infections: A multicenter study. Radiology 2022;303:682-692.
11.
Masci
GM, Izzo A, Bonito G, et al. Chest CT features of COVID-19 in vaccinated versus
unvaccinated patients: use of CT severity score and outcome analysis. La
radiologia medica 2023:128(8):934-943.
12.
Statsenko
Y, Al Zahmi F, Habuza T, et al . Impact of age and sex on COVID-19 severity
assessed from radiologic and clinical findings. Front Cell Infect Microbiol
2022;11:1395.
13.
Zovi
A, Ferrara F, Langella R, Cavallaro F, Vitiello A. Sex affects immune response
capacity against COVID‐19 infection. Rev Med Virol 2023:33(4):2450.
14.
Verma
A, Kumar I, Singh PK, A et al. Initial comparative analysis of pulmonary
involvement on HRCT between vaccinated and non-vaccinated subjects of COVID-19.
Eur Radiol 2022;32(6):4275-4283.
15.
Vishwanath
T, Rajalakshmi BR, Sadananda KS, Manjunath CN. Association of Chest CT Severity
Scores and Vaccination Status in COVID-19 Disease: A Cross-sectional Study. J
Clin Diagn Res 2022;16(2).
16.
Carbonaro
L, Braga F, Gemma P, et al. Chest computed tomography of suspected COVID-19
pneumonia in the Emergency Department: comparative analysis between patients
with different vaccination status. Pol J Radiol 2023;88(1):80-88.
17.
Sharma
R, Thakker V, Sharma RB, Arora M, Sarda P, Ahuja M, Randhawa LS, Azad RK.
Effect of vaccination on the HRCT profile of COVID-19 patients-A single-center
experience. J Fam Med Prim Care 2022;11(6):2938.