Cough-Induced Rib Fracture in a Healthy Woman: A Case Report
ABSTRACT
Background: Only a few cases
of cough-induced rib fracture have been described in the medical literature.
The impact of decreased bone mineral density (BMD) on traumatic rib fractures
remains unknown. In this study, we presented a case of
a healthy 41-year-old female patient who was detected to have cough-induced rib
fracture during the evaluation of symptoms of chronic cough with pleuritic
chest pain. The patient developed left sixth and
ninth rib fractures, after severe coughing for three months secondary to upper
respiratory tract infection. The patient was treated conservatively with good
clinical outcome. Conservative treatment is the first-choice approach except in
cases of complications when the surgical approach should be considered.
Cough-induced rib fracture should be remembered as a possible diagnosis, as
diagnostic delays increase the risk of complications.
Keywords:
Rib fracture; Cough; Chest pain, Spontaneous fracture;
Bone mineral density
INTRODUCTION
Coughing
is considered an important physiological
defense mechanism that is often self-limited and uncomplicated. However,
when severe, it can be associated with pneumothorax, pulmonary herniation, or
rib fractures1,2. Most commonly, rib
fractures are caused by a thoracic injury. Infrequently, after the onset of
coughing, patients presenting with persistent chest pain are found to have rib
fractures3. Studies so far showed
that cough-induced rib fractures occurred most frequently on the lateral side
of the fifth through ninth ribs1,
with the sixth rib being the most common site4.
CASE PRESENTATION
We presented a case of
a healthy 41-year-old female patient who was detected to have cough-induced rib
fracture during the evaluation of symptoms of chronic cough with pleuritic
chest pain who developed left sixth and ninth rib
fractures, after severe coughing for three months secondary to upper
respiratory tract infection. A
41-year-old female presented to the pulmonologist complaining of respiratory
discomfort, pain in the left chest, and non-productive cough, in the duration
for three months. Three months ago she had an upper respiratory tract
infection. Since then, she has had an
irritating, non-productive cough, and she felt pain in the lower part of the
chest during more intense coughing, more pronounced on the left side. During
seven days before the examination, the pain increased and was more pronounced
when touching the left chest wall, and when taking a deep breath. She used
analgesic therapy as needed. The patient denies any recent chest injury, and is
healthy so far. Physiological functions are normal. She is a non-smoker and
does not consume alcohol. The patient does not take any drug for any chronic or
acute disease.
On clinical examination was eupnoic, with normal
body temperature at 36.5 *C, acyanotic (SpO2: 95%), with normal blood pressure
(120/70 mmHg). Physical examination revealed no remarkable findings except for
tenderness upon palpation of the left chest wall, mainly in the left lower
quadrant. Lungs auscultation showed normal findings without crepitation and
wheezing. Blood tests were performed. A complete blood count and a metabolic
panel ruled out anemia or plasma cell dyscrasia. Liver function tests, serum creatinine
tests, thyroid function tests, parathyroid hormone, 25-hydroxy vitamin D
levels, showed no abnormal findings except for a low vitamin D level. Blood
calcium measurement and other relevant studies performed to rule out secondary etiologies
of pathological rib fracture were unchanged.
Table 1. Laboratory findings.
|
Investigation |
Value |
Reference range with unit |
|
WBC
|
5.4 |
3.4–9.7
x× 109/L |
|
Hemoglobin
|
133 |
138–175
g/L |
|
Creatinine |
70 |
49–104
umol/L |
|
Calcium |
2.42 |
2.14–2.53
mmol/L |
|
CRP |
1.0 |
0.0–5.0
mg/L |
|
AST |
16 |
11–38
U/L |
|
ALT
|
29 |
12–48
U/L |
|
LDH |
155 |
124-241
U/L |
|
GGT |
18 |
9–35
U/L |
|
ALP |
84 |
54–119
U/L |
|
25-hydroxy vitamin D |
46.7 |
75–100
nmol/L |
|
Total
proteins |
74.2 |
66–81
g/L |
|
Albumin |
47.1 |
40.6–51.4
g/L |
|
TSH |
5.12 |
0.465–4.68
mIU/L |
|
T4 |
14.9 |
10.0–28.2
pmol/L |
|
PTH |
51.7 |
15.0–68.3
pg/mL |
Abbreviations: WBC, white
blood cell; CRP, C-reactive protein; AST, aspartate aminotransferase; ALT,
alanine transaminase; LDH, lacticacid dehydrogenase; GGT,
gamma-glutamyltransferase; ALP, alkaline phosphatase; TSH,
thyroid-stimulating hormone; T4, thyroxine; PTH, parathyroid hormone
METHODS (DIFFERENTIAL
DIAGNOSIS, INVESTIGATIONS, AND TREATMENT)
The chest X-ray posteroanterior (PA) and oblique radiograph
projection view
showed in the lateral part of the left sixth and
ninth rib, visible fractures without
major displacement of the bone fragments. There are no signs of pneumothorax.
Lung parenchyma and bronchial wall thickness were normal (Figure 1). 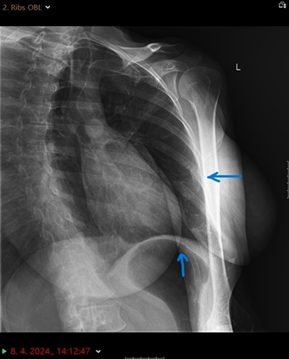

Figure 1. (A) Radiological image of the thorax. Chest oblique and
posteroanterior radiograph projection view
(B). The blue arrow points an visible fractures of the left sixth and ninth
ribs.
Osteodensitometry results showed signs of reduced bone mineralization at the level of
osteopenia with the recommendation of antiresorptive treatment. The patient was examined by the thoracic surgeon
who recommended conservative treatment, and the patient was discharged after
pain control and supportive measures with antitussives and nonsteroidal
anti-inflammatory drugs, and slowly improved. For chest pain, the patient was
administered simple analgesia consisting of codeine phosphate, and
acetaminophen. One month later, the patient completely recovered, and was
symptom-free with no chest pain and with a complete normal examination with no
pain in the ribs.
DISCUSSION
Cough-induced
rib fracture is a very rare condition, with a few cases described in the
medical literature5. Rib fractures may occur with chronic cough following chronic obstructive
pulmonary disease, or bronchial asthma under steroid therapy. These were
concluded to be risk factors for cough-induced rib fracture6. According to current knowledge, in most patients, the fracture is
solitary (64.3%), and Sano et al. described the right side as the most common
location (57%), especially the right tenth rib (42.8%)4. In our case, both fractured ribs
were on the left side. The impact of decreased bone mineral density
(BMD) on traumatic rib fractures remains unknown7. Conservative
treatment is the first-choice approach. The surgical approach should be
considered in cases of daily activities limiting symptoms (e.g. pain, dyspnea)
or complications, such as pulmonary herniation, pneumothorax, or diaphragmatic
laceration8, 9.
CONCLUSION
Our
study showed sixth and ninth cough-induced rib fractures in a healthy female
patient without an underlying predisposition. The only pathological finding
recorded in our patient was mild osteopenia. It is important to remember this
cause of pain after chronic cough, in the case of healthy individuals as a
possible diagnosis. In conclusion, timely establishment of the diagnosis
decreases the risk of complications, such as chronic pain and rupture of
organs.
Declarations
Authors' contributions: Tanja Zovko: Conceptualization; visualization; writing –
original draft; writing – review & editing. Kristina Galic:
Methodology; supervision; validation. Marina Vasilj: Data curation; writing; project administration. Marija
Goluza Sesar: Investigation; resources. Stanko Zovko:
Resources; software. Miro Mandić: Data
curation; formal analysis.
Author Disclosure Information:
Authors state no conflict of interest.
Research funding:
Authors state no funding involved.
Patient consent statement: The signed informed consent was obtained from the patient
for the publication of the case report.
REFERENCES
2. Trovato
DA, Sousa JE, Bruetman JE, Finn BC, Young P. [Symmetrical rib fractures
associated with chronic cough: report of one case]. Rev Med Chil
2018;146(3):391-393.
3. Hanak
V, Hartman T, Ryu J. Cough-induced rib fractures: review of 54 cases. Chest
2005;12(4).
4. Sano
A, Tashiro K, Fukuda T. Cough-induced rib fractures. Asian Cardiovasc Thorac
Ann 2015;23(8):958-960.
5. Bezerra
LS, Barbosa da Silva GS, Santos-Veloso MAO, Bosford MAP, Carvalhoco ARMR.
Clinical and Radiological Aspects of Cough-induced Rib Fractures: A case
report. Cureus 2020;12(2):6840.
6. Sakellaridis
T, Andrianopoulos E, Stamatelopoulos A, Laoutides G, Kormas P. Cough induced
rib fractures in patients with respiratory infection. Chirurgia 2008;21(2):73-76.
7. Tang
Y, Hong W, Xu X, Li M, Jin L. Traumatic rib fracture patterns associated with
bone mineral density statuses derived from CT images. Front Endocrinol
(Lausanne) 2023:14:1304219.
8. Katrancioglu
O, Akkas Y, Arslan S, Sahin E. Spontaneous rib fractures. Asian Cardiovasc
Thorac Ann 2015;23(6):701-703.
9. Parks
RM, Jadoon M, Duffy J. Nontraumatic rupture of the costal margin: a
single-center experience. Asian Cardiovasc Thorac Ann 2019;27(2):105-109.