Diagnostic Dilemma: A Case of Necrotizing Neutrophilic Dermatosis Misdiagnosed as Necrotizing Fasciitis
Abstract
We report the case of a 15-year-old female who presented with a necrotizing neutrophilic dermatosis (nnd) following an unknown insect bite on her right leg. Initially misdiagnosed, she developed sepsis and required intermediate care for acute kidney injury and volume support. Through multidisciplinary collaboration between pediatrics, infectious diseases, dermatology, and plastic surgery teams, the diagnosis of nnd was suspected and confirmed via skin biopsy. She was successfully treated with corticosteroids and wound care, avoiding surgical intervention typically required for necrotizing fasciitis (nf). This case highlights the importance of considering nnd in the differential diagnosis of progressive inflammatory skin lesions and emphasizes the value of conservative management to prevent iatrogenic complications.
Categories: plastic surgery; dermatology; allergy/immunology
Introuction
Neutrophilic dermatoses (nds) are rare inflammatory skin disorders characterized by neutrophilic infiltration without identifiable infection1. Their clinical presentations vary, including vesicles, papules, nodules, ulcerations, or extracutaneous involvement2. The etiology of nds is often idiopathic and poorly understood3. These conditions can resemble necrotizing fasciitis (nf), posing a diagnostic challenge due to overlapping clinical features2,4. Pathergy-a hypersensitivity reaction to trauma-is a hallmark of nds, where procedures such as biopsies or injections can exacerbate lesions4. Misdiagnosing nds as nf and proceeding with surgical interventions may result in significant iatrogenic harm. Early recognition of nds, supported by biopsy and imaging findings, is crucial for optimal management5,6. This report describes a challenging case of nnd initially mistaken for nf.
Case presentation
A healthy 15-year-old girl presented to a peripheral healthcare center with extensive cellulitis of the right leg after a suspected insect bite. Symptoms included fever (>38°c), erythema, swelling, and inability to walk. She was treated with amoxicillin/clavulanic acid and admitted for monitoring. Despite treatment, her condition worsened, with circumferential leg inflammation, exudative papules, and systemic inflammatory signs, as shown in below (figure 1).

Figure 1: skin lesions at admission
Vesicles and necrotic papules of the right leg, two weeks since symptoms onset
Transferred to our center two weeks after symptoms onset, she exhibited sepsis, acute kidney injury, bilateral pleural effusion, and hemorrhagic blisters. Laboratory tests showed leukocytosis and coagulopathy (platelets: 87,000/μl, inr: 2.38, fibrinogen: 141 mg/dl). Complete blood test results are shown below (table 1).
Table 1: blood test results
|
Blood test |
Result |
Normal
value |
|
Rbc |
2.63 x 10^12/l |
3.8-5.1 |
|
Hemoglobin |
8.6 g/dl |
12.0-15.3 |
|
Hematocrit |
25.4 % |
36.0-46.0 |
|
Wbc |
14.60
x10^9/l |
4.0-11.0 |
|
Neutrophils |
73.4 / 10.72 % |
1.9-7.5 . |
|
Monocytes |
8.8 / 1.28
% |
0.1-1.0 . |
|
Platelets |
78 x10^9/l |
150-450 |
|
Inr |
2.33 |
|
|
Urea |
36 mg/dl |
16 - 49 |
|
Creatinine |
1.24 mg/dl |
0.50-0.90 |
|
Albumin |
1.9 g/dl |
3.5 - 5.2 |
|
Crp |
6.75 mg/dl |
<0.5 |
Cultures remained negative, and broad-spectrum
antibiotics were administered. A ct scan ruled out nf, showing infection
confined to subcutaneous tissue without fascial involvement, specifically
absence of deep plane infiltration, emphysema or organized collections (figure 2).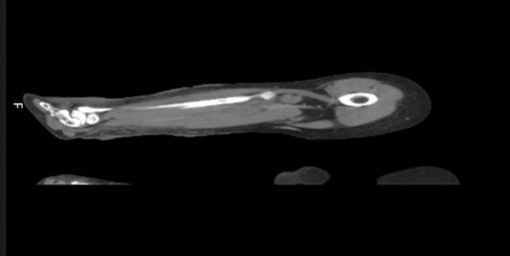
Figure 2:
ct scan of right leg Signs of subcutaneous
tissue densification without collections or deep-tissue gas formation
Multidisciplinary discussions among pediatrics, infectious
diseases, dermatology and plastic surgery teams deferred surgical debridement.
A skin biopsy was performed to investigate nds and corticosteroids
(prednisolone 30 mg iv every 12 hours) were initiated. Wound care included
flaminal®, allevyn® and mepilex® dressings (figure 3).
Figure 3:
wound care Progressive resolution of
skin lesions with frequent dressings
Over two weeks, the patient’s condition improved.
Biopsy results confirmed nnd, showing neutrophilic infiltrate, vasculitis and
necrosis. After 45 days of hospitalization, the patient was discharged on
prednisolone and cyclosporine, with follow-up care. Scarring was evident but
improved progressively (figure 4).
Figure 4:
8 months after hospital discharge
Secondary healing with
scarring of previous wounds
Discussion
Diagnosing
nds is challenging due to their rarity and clinical overlap with nf1,7. Both conditions present with progressive
skin lesions, fever, leukocytosis, and systemic inflammatory markers involving
necrosis of tissues8,9.
Distinguishing between these entities is crucial for appropriate treatment, as
one is primarily infectious and the other is inflammatory. Nf, however, often
involves deep tissue destruction and requires emergent surgical debridement10,11. In contrast, nds are treated with
systemic corticosteroids and conservative wound care10,12. Pathergy is a key differentiator, as
trauma-induced lesions in nds may worsen with surgical interventions8.
Nf
is infectious in origin, often followed by trauma and caused by bacteria as
streptococcus pyogenes, staphylococcus aureus (including mrsa), clostridium
species, or polymicrobial infections11,13.
Clinical presentation is a rapidly progressing infection of the fascia and
subcutaneous tissue with systemic toxicity, severe pain out of proportion, skin
changes with eventual necrosis, fever, tachycardia, hypotension and multi-organ
dysfunction in advanced cases11,13.
Bacterial toxins and enzymes cause tissue destruction, vascular occlusion and
necrosis and systemic inflammatory response can lead to septic shock13.
Histopathology
shows necrosis with neutrophilic infiltration and presence of bacteria in
tissue samples. Surgical exploration for confirmation and positive cultures is
the current diagnostic criteria13.
Treatment needs emergent surgical debridement, broad-spectrum antibiotics and
supportive care7,11,13.
Nnd
is an inflammatory condition, non-infectious in nature associated with immune
dysregulation or underlying systemic or inflammatory disorders9. Clinical presentation is a progressive
painful skin necrotic plaques, nodules or ulcers, resembling nf but without signs
of systemic infection6,10.
Immunemediated neutrophilic infiltration cause tissue necrosis without pathogen
involvement and histopathology shows neutrophilic infiltrate with tissue
necrosis without organisms5,9.
Diagnosis is based on clinical suspicion with exclusion of infectious causes
such as nf and biopsy with absence of infection and no microbial growth2,6,12. Treatment involves high-dose systemic
corticosteroids, immunosuppressive agents as cyclosporine and treatment of underlying
systemic disease9,10.
Key
diagnostic differences listed in table below (table 2)5,6,9,13
Table 2:
key diagnostic differences between nf and nnd
|
Feature |
Necrotizing
fasciitis |
Necrotizing
neutrophilic dermatosis |
|
Cause |
Infectious (bacterial) |
Non-infectious (immune-mediated) |
|
Systemic signs |
Prominent
(fever, hypotension, sepsis) |
Mild or
absent; prominent in advanced cases |
|
Pain |
Severe and out of proportion |
Severe but more localized |
|
Tissue involvement |
Deep
fascia and subcutaneous tissue |
Dermis
and subcutaneous tissue |
|
Cultures |
Positive (bacteria detected) |
Negative (sterile) |
|
Histopathology |
Neutrophils
with bacterial presence |
Neutrophils
without bacteria |
|
Treatment |
Surgical debridement, antibiotics |
Corticosteroids, immunosuppressants |
Accurate diagnosis often requires tissue biopsy, culture, and imaging to distinguish between these two entities, as the treatment strategies are fundamentally different.
In this case, imaging findings, slow disease progression and multidisciplinary collaboration helped avoid unnecessary surgery. Early corticosteroid therapy supported the diagnosis, with the patient showing rapid improvement.
This case emphasizes the importance of a multidisciplinary approach, especially involving dermatology teams, to navigate ambiguous clinical presentations and reduce morbidity.
Conclusion
This case underscores the diagnostic complexity of nnd and the importance of distinguishing it from nf.
High clinical suspicion and conservative management can prevent iatrogenic complications.
Multidisciplinary collaboration and early biopsy are essential for accurate diagnosis and effective treatment. Awareness of nnd as a differential diagnosis for necrotizing skin lesions may improve outcomes and reduce unnecessary surgical interventions.
Disclosures
Human subjects: consent for treatment and open access publication was obtained or waived by all participants in this study. Conflicts of interest: in compliance with the icmje uniform disclosure form, all authors declare the following: payment/services info: all authors have declared that no financial support was received from any organization for the submitted work. Financial relationships: all authors have declared that they have no financial relationships at present or within the previous three years with any organizations that might have an interest in the submitted work. Other relationships: all authors have declared that there are no other relationships or activities that could appear to have influenced the submitted work.
References
3. kobayashi sd, malachowa n, deleo fr. Neutrophils and bacterial immune evasion. J innate immun 2018;10(5-6):432-441.
4. shah n, asdourian ms, jacoby tv. Neutrophilic dermatosis and management strategies for the inpatient dermatologist. Current dermatology reports 2022;3:146-157.
5. nelson ca, stephen s, ashchyan hj, james wd, micheletti rg, rosenbach m. Neutrophilic dermatoses:
Pathogenesis, sweet syndrome,
neutrophilic eccrine hidradenitis, and behçet disease. J am acad dermatol 2018;79(6):987-1006.
6. sanchez im, lowenstein s: johnson ka. Clinical
features of neutrophilic dermatosis variants resembling necrotizing fasciitis.
Jama dermatol 2019;155:79-84.
7. wong ch, yam akt, tan abh. Approach to
debridement in necrotizing fasciitis. Am j surg 2008;196(3):19-24.
8. Rahman s, daveluy s. Pathergy
test. Treasure island (fl). Statpearls publishing, 2022.
9. kroshinsky d, alloo a, rothschild b. Necrotizing
sweet syndrome: a new variant of neutrophilic dermatosis mimicking necrotizing
fasciitis. J am acad dermatol 2012;67(5):945-954
10. gowda a, christensen l,
polly s. Necrotizing neutrophilic dermatosis: a diagnostic challenge with a
need for multi-disciplinary recognition, a case report. Annals of medicine and
surgery, 2020; 57:299-302.
11. allaw
f, wehbe s, kanj ss. Necrotizing fasciitis: an update on epidemiology,
diagnostic methods, and treatment. Curr opin infect dis, 2024; 37:105-111.
12. su wp, liu hn. Diagnostic
criteria for sweet's syndrome. Cutis, 1986; 37:167-174.
13. misiakos
e, bagias g, patapis p. Current concepts in the management of necrotizing
fasciitis. Frontiers in surgery, 2014; 1: 36.