Eufunctioning Benign Intrathoracic Goiter
Abstract
Intrathoracic goiter is an entity in which the thyroid gland increases in size and is partially or completely located in the mediastinum. Symptoms can vary because it depends on the volume and extent, but include dyspnea, cough, dysphonia or dysphagia. In some cases, they are very well tolerated and when patients consult, they are of significant size. Most of them are accompanied by normal thyroid function. Treatment is carried out according to the presence or absence of obstructive symptoms. Three clinical cases are presented, in which the first two had obstructive elements, one of which required oxygen and the other was totally asymptomatic.
Introduction
The majority are eufunctioning, that is, they are accompanied by normal thyroid function; but in a small percentage they present as hyper or hypo functioning4,5.
Due to its location, it can cause venous, nervous, esophageal and/or tracheo-bronchial compression, especially in long-lasting goiters. Compressive symptoms appear as obstruction due to progressive compression of the trachea or the sudden enlargement of a thyroid nodule that has bled into it.
The diagnosis can be clinical, when goiter is detected in the physical examination, or imaging when visualized in ultrasound, tomography or magnetic resonance studies.
After the discovery of goiter, biochemistry is requested to evaluate thyroid function and seek to identify the cause that produces it and determine if there are obstructive symptoms.
The treatment of choice may be surgical, with the excision of part or all of the gland, but rather radioactive iodine in specific cases or expectant management. After surgery has been determined as a treatment, complementary studies should be requested if necessary and laryngoscopy to visualize the tracheal lumen and the vocal cords.
Ideally, definitive treatment should be carried out before symptoms or comorbidities appear in the patient that may prevent surgery. In the case of patients with minimally substernal goiters, the goal is to treat them before the goiter spreads to the chest6.
Clinical cases
Case 1
A 59-year-old woman, former smoker, with a history of subarachnoid hemorrhage secondary to cerebral aneurysm, chronic obstructive artery disease and osteoporosis.
She was evaluated during hospitalization for multinodular goiter, which resulted in severe tracheal stenosis and respiratory failure, with compressive elements (functional class iii dyspnea, dysphagia for solids, and dysphonia). She had a goiter diagnosed 20 years ago, without regular check-ups.
On physical examination, she had a grade iv goiter, the lower edge could not be palpated, and collateral circulation was observed in the upper hemithorax (figure 1). The maranon-pemberton maneuver was positive. No elements of ophthalmopathy were found. The ultrasound showed an enlarged thyroid gland of 90 cc, with multilobed edges, a heterogeneous echo structure at the expense of multiple mixed nodules predominantly spongiform; the smaller ones measured between 5 and 9 mm and had a diffuse distribution. The two largest were located in the right lobe, measuring 22 x 15 mm and 35 x 24 mm. The gland had preserved vascularization, which determined compression of the airway.

Figure 1: redness or facial flushing that is accompanied by thoracic varicose veins due to engorgement, a product of compression and slave edema.
The computed tomography (ct) showed an increase in the size of the thyroid with an estimated volume of 100 cc, with intrathoracic extension at the expense of multiple nodules. The largest one was 35 mm, with a cystic appearance, with macrocalcifications located in the ld, which correlates with the ultrasound description. Extrinsic compression was determined in the upper third of the trachea, with a residual lumen of 3 mm x 14 mm (figures 2 and 3).
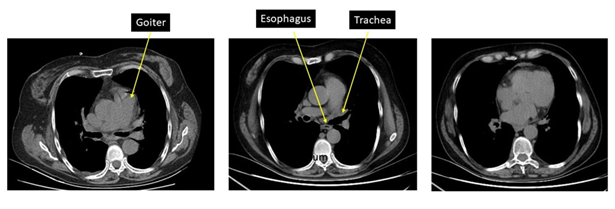
Figure 2: ct, axial section showing substernal goiter with displacement and narrowing of the tracheal lumen and the esophagus
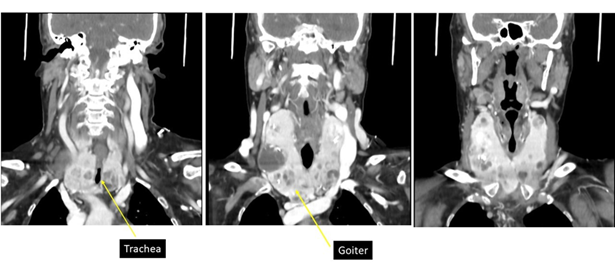
Figure 3: ct, coronal section in which a large multinodular goiter with a cystic area is observed and in the image on the right tracheal light compression with an "hourglass" image
Tsh was 19 µu/ml (0.5 -4.7). Due to the patient's obstructive symptoms, she required oxygen for adequate saturation. Methimazole was discontinued, liothyronine 10 mg every 12 hours for 5 days was started, and eu function was achieved so that she underwent total thyroidectomy, which was performed without complications.
Pathology showed a gland with a smooth, polylobed external surface, weighing 182 grams, with multiple colloid-like nodules, with a calcified area and a degenerative appearance between 30 and 40 mm. Microscopically, a nodular lesion with a follicular architecture, not encapsulated, well-defined, composed of follicular cells without nuclear atypia or mitosis; stroma with areas of hyalinization and fibrosis, scant inflammatory exudate without formation of aggregates or lymphoid follicles.
The patient required an oxygen mask to achieve adequate oxygen saturation.
As a post-surgical complication, she presented transient hypoparathyroidism. Upon discharge, the patient's respiratory failure showed clear improvement and levothyroxine was started at 1.6 ug/kg/day, with subsequent controls in the outpatient clinic.
Case 2
Woman, 63 years old, obese, hypertensive, former heavy smoker; assessed in a polyclinic for grade iv goiter accompanied by progressive dyspnea (currently functional grade iii - iv), of two years' duration. In the previous month, she added cough when lying down and dysphonia. No clinical elements of thyroid dysfunction.
The ultrasound showed a thyroid gland with a heterogeneous echo structure, with an estimated volume of 91 cc. The left lobe is replaced by a voluminous solid mass, with defined margins, with a heterogeneous echo structure at the expense of multiple macrocalcifications inside.
The ct showed a voluminous mass with an epicenter in the li measuring 62 x 72 x 53 mm. On its right lateral side, it contacts and displaces the visceral axis of the neck. It determined stenosis of the trachea with a residual lumen of up to 9 mm (figures 4 and 5).
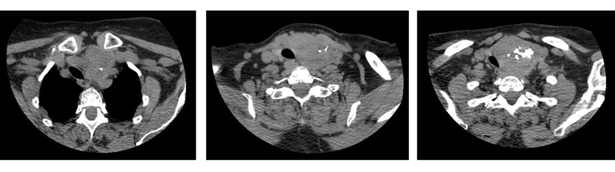
Figure 4: ct, axial section showing goiter mainly in the left lobe with displacement of the visceral axis of the neck and tracheal lumen stenosis
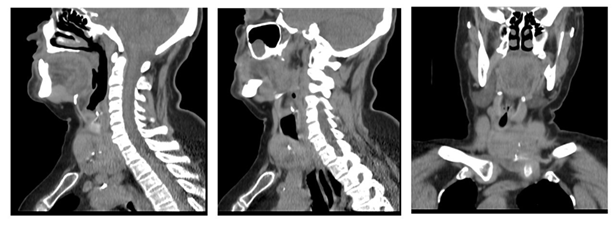
Figure 5: ct, sagittal and coronal section showing substernal goiter extending below the brachiocephalic vessels with displacement and narrowing of the tracheal lumen Thyroid function was normal.
Total thyroidectomy was performed, and transient hypoparathyroidism was a complication. Upon discharge, the patient was asymptomatic, under treatment with full dose levothyroxine and 3 grams of calcium plus 0.50 mg of calcitriol, which was then discontinued due to resolution of hypoparathyroidism.
Case 3
A 48-year-old man with a personal history of schizophrenia, who consulted because a family member had noticed an increase in the anterior face of the neck in recent days. He denied locoregional compressive elements, nor symptoms of thyroid dysfunction. The examination revealed a grade iii goiter with a firm elastic consistency. From the laboratory tsh: 12.7 µu/ml (0.5 -4.7); it was repeated and the tsh was 3.27 with ft4 of 0.90 (normal).
The neck ultrasound showed an enlarged thyroid gland, with an estimated volume of 84cc, ld of 50cc, li 34cc. It has a slight intrathoracic component, predominantly on the right. Its echo structure is heterogeneous, at the expense of multiple bilateral hypo-echoic areas that give it a seudonodular appearance, as can be seen in chronic thyroiditis. Solid, hyperechoic, well-defined nodule, with a fine peripheral halo, without vascularization on color doppler, 13 mm x 16 mm x 17 m l, t, ap.
The ct of the neck reported: multinodular goiter with intrathoracic extension from the operculum 19 mm, volume 71 cc. Visceral axis of the neck well centered. No alterations are observed in the walls of the pharynx. Fatty spaces for pharyngeal muscles preserved (figure 6).
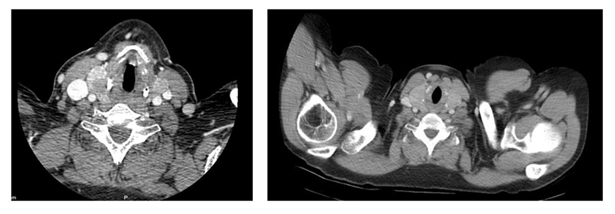
Figure 6: ct with goiter that maintains undamaged tracheal lumen.
Discussion
Intrathoracic or plongeant goiter represents about 5.8% of intrathoracic masses7. It occurs when its structure is located at least 50% within the mediastinum, at the level of the prevascular or retrovascular space, reaching the aortic arch. Most of the time it is a benign mass found in the anterior mediastinum8,9.
Substernal goiter can be detected incidentally in a chest x-ray or ct scan or it can be found due to obstructive elements such as dyspnea, wheezing or cough. The most common obstructive symptom is dyspnea on exertion, which is present in 30 to 60% of cases. It usually occurs when the tracheal diameter is less than 8 mm6.
Plongeant goiter is more frequent in women, with an age at diagnosis between the fourth and fifth decade of life. Most are benign and their main etiology is multinodular goiter, followed by follicular adenoma and hashimoto's thyroiditis8. More than 70% are eufunctioning, between 20 - 30% are described as hyperfunctioning, the most common cause being the automatization of thyroid nodules larger than 3 cm10-13.
Clinical manifestations depend on the size of the goiter, its etiology and the adjacent structures involved. The most frequent symptoms, due to compression of the adjacent structures, are respiratory, digestive, vascular and nervous5.
Dyspnea, cough, laryngeal stridor and dysphonia are the main respiratory symptoms5. Superior vena cava syndrome and its thrombosis are presented as vascular symptoms5: nerve compression can cause bitonal voice, claude bernard-horner syndrome or paralysis of the hemidiaphragm14; esophageal compression causes progressive and permanent dysphagia5.
On physical examination, a mass is palpated at the cervical level, without being able to palpate the lower edge of the thyroid gland. The maranon-pemberton sign (facial plethora caused by compression of the vasculature at the level of the thoracic operculum when the upper limbs are raised) may be present3,5.
To complement the assessment, imaging tests are used to determine the extent of the goiter and laboratory tests to assess its functionality.
Functional assessment is performed by measuring thyroid stimulating hormone (tsh), which can determine whether the goiter is eu functional or accompanied by hypo or hyperfunction.
Thyroid ultrasound is the test of choice for assessment of the thyroid gland, and should be requested as an initial approach. It is a noninvasive, cost-effective and operator-dependent study. It reveals important data such as glandular volume, presence of nodules and their characteristics. Since neck ultrasound cannot assess the intrathoracic portion of the goiter, it is complemented by other imaging tests such as x-ray and ct of the neck and chest1,4.
Neck and chest x-ray are a widely available test and can be used as one of the first steps in radiological assessment. In this, a mass can be observed at the level of the mediastinum, the diameter of the trachea is measured and it is determined whether or not there is displacement of the trachea1,5.
Ct with contrast provides us with more precise information, such as the extent of the goiter, its relationship with the intrathoracic organs, diameter of the tracheal lumen and its displacement, these being important to decide the surgical approach and the extent of the surgery15,16.
The treatment of intrathoracic goiter will depend on the presence of obstructive symptoms. In patients with obstructive symptoms (dysphagia, dyspnea, cough) they require removal or ablation of the thyroid, given that once they appear, there is a greater risk of thyroid growth and progressive tracheal compression, which in some cases (such as hemorrhage) can be rapid and cause death6.
Surgery is preferred because it eliminates the goiter and provides immediate relief of obstructive symptoms, whereas radioactive iodine only moderately reduces thyroid volume (40 to 60%)17,18.
In the case of intrathoracic goiter without obstructive elements, treatment depends on the degree of substernal extension and the characteristics of the patient6- the indication of surgical treatment in these cases is debatable. There are authors who do not recommend it due to the possible risks of complications in patients who would not improve in their normal life by not having symptoms.
Cases that propose surgical treatment in asymptomatic patients justify this conduct by certain facts such as that the passage of time converts the same person with more comorbidities and more susceptible to complications; that the intrathoracic component could hide a cancer or cause bleeding from a nodule and generate acute respiratory distress.
The extent of surgery for benign goiter depends on the
extent of the goiter and whether the patient has symptoms. Due to the risk of
recurrence, a total or almost total thyroidectomy is recommended, unless during
surgery a higher risk of injury to the recurrent laryngeal nerve or
complications is observed6.
Regarding the surgical technique, most obstructive and
intrathoracic goiters can be removed through a standard cervical (arcuate)
incision19,20, although in
certain cases sternotomy or thoracotomy may be required in patients with a
previous thyroidectomy, very large substernal goiters or invasive cancer21.
The most frequent postoperative complications are
transient hypoparathyroidism, permanent hypoparathyroidism, hemorrhage, wound
infection, injury to the recurrent laryngeal nerve, and tracheomalacia. These
complications are reduced if the surgery is performed by an experienced surgeon
in a center with a high flow of patients1.
Tracheomalacia is the weakness or destruction of the trachea caused by the
pressure exerted by the goiter on the tracheal rings, which weaken it and cause
its collapse in the postoperative period. If it is recognized at the time of
surgery, tracheomalacia can, in some cases, be treated by partial tracheal
resection and reconstruction; otherwise, a tracheotomy is necessary6.
Iodine 131 can be used in patients with obstructive
symptoms who are a poor candidate for surgery or who wish to avoid surgical
risks, and especially in patients who are accompanied by hyperthyroidism. Some
cases of post-radiation thyroiditis induced by radioactive iodine with acute
worsening of airway obstruction have been described6.
There is still little evidence to support the
treatment of this type of goiter with thermal ablation.
In the first two cases presented, the obstructive
symptoms were decisive for the indication of thyroidectomy and in the first, to
compensate for respiratory failure, an oxygen mask was required; this is rare.
In the third case, no treatment has been indicated because the patient remains
asymptomatic.
References
1. pazos b, bonilla g,
montero m. Bocio intratorácico. Revista médica sinergia 2020;5(10):1-11.
2. martinez
z, agüero p, mintegui g. Plongeant goiter short case series description. Clinical
reviews and case reports 2023;2(2):1-5.
3. Argente horacio a. Semiología medica: fisiopatologia. Semiotecnia y
propedéutica / horacio a. Argente; marcelo alvarez - 3a ed - ciudad autónoma de
buenos aires: médica panamericana, 2021.
4. durante c, hegedüs l,
czarniecka a, paschke r, russ g, schmitt f, soares p, solymosi t, papini e.
European thyroid association clinical practice guidelines for thyroid nodule
management. Eur thyroid j 2023;12(5):1-22.
5. mainetti m. Bocio intratorácico. Congresos uruguayos de
cirugía 1955;174-187.
6. Ross ds,
cooper ds, mulder je, treatment of benign obstructive or substernal goiter.
Uptodate: fecha de acceso 10 de diciembre de 2024.
7. jiménez-lópez m, gómez-hernández m. Tiroides
endotorácico. Indicaciones del abordaje endotorácico. Rev.
Orl 2020;217-223.
8. di crescenzo v, vitale m, valvano l, napolitano f,
vatrella a, zeppa p, et al. Surgical management of
cervico-mediastinal goiters: our experience and review of the literature. Int j
surg 2016;28:47-53
9. carrillo-esper r, carrillo-córdova dm, cabello-aguilera
r. Bocio intratorácico normofuncionante. Med int méx
2020;36(1):265-271.
10. cappellacci f, canu gl, rossi l, et al. Differences
in surgical outcomes between cervical goiter and retrosternal goiter: an
international, multicentric evaluation. Front surg 2024;11:1-6.
11. torre g, borgonovo g, amato a, et al. Surgical
management of substernal goiter: analysis of 237 patients. Am surg
1995;61(9):826-831.
12. chow
tl, chan tt, suen dt, chu dw, lam sh. Surgical management of substernal goitre:
local experience. Hong kong med j 2005;11(5):360-365.
13. aghajanzadeh
m, asgary mr, mohammadi f, darvishi h, safarpour y. An investigation into
symptoms, diagnosis, treatment, and treatment complications in patients with
retrosternal goiter. J family med prim care 2018;7(1):224-229.
14. pérez-aguirre e, sánchez-pernaute a, gonzález o, hernando
f, díez-valladares l, torres a, & balibrea j. Síndrome de claude
bernar-horner, parálisis recurrencial e insuficiencia respiratoria aguda
secundarias a adenoma folicular de tiroides. Cirugía española
2001;69(4):401-403.
15. ríos a, sitges-serra a. Tratamiento quirúrgico del bocio
intratorácico. Cirugía española 2012;90:421-428.
16. Jiménez-lópez m, gómez-hernández m. Tiroides endotorácico. Indicaciones del
abordaje endotorácico. Revista orl, 2020;11:217-223.
17. bonnema sj, hegedüs l.
Radioiodine therapy in benign thyroid diseases: effects, side effects, and
factors affecting therapeutic outcome. Endocr rev 2012;33(6):920-980.
18. villadsen mj, sørensen
ch, godballe c, nygaard b. Need for thyroidectomy in patients treated with
radioactive iodide for benign thyroid disease. Dan med bull 2011;58(12):1-4.
19. hegedüs l, bonnema sj.
Approach to management of the patient with primary or secondary intrathoracic
goiter. J clin endocrinol metab 2010;95(12):5155-62.
20. nakaya m, ito a, mori a, et al. Surgical
treatment of substernal goiter: an analysis of 44 cases. Auris nasus larynx
2017;44(1):111-115.
21. wong wk, shetty s, morton
rp, mcivor np, zheng t. Management of retrosternal goiter: retrospective study
of 72 patients at two secondary care centers. Auris nasus larynx
2019;46(1):129-134.
22. chen ay, bernet vj, carty
se, et al. American thyroid association statement on optimal surgical
management of goiter. Thyroid 2014;24(2):181-189.