Hepatic Tuberculosis: A Case Report
Abstract
The primary form of hepatic tuberculosis, is rather rare, often has misleading appearances. Its diagnosis is histological and/or bacteriological. We report the case of a 38-year-old woman, with a history of mental retardation since childhood, who consulted for acute pain in the right hypochondrium. Abdominal ultrasound showed a thin-walled vesicle containing several microstones. On the thoraco-abdominopelvic scan with opacification, there was cholecystitis with a heterogeneous liver with multiple rounded hypodense microlesions, slightly enhanced after injection of contrast product and the abdominal mri showed isointense t1-t2 hepatic micronodules. The etiological search for this hepatic granulomatosis including an assessment of autoimmunity, sarcoidosis was negative, as well as the infectious causes were eliminated. A laparoscopy was carried out with a cholecystectomy. The exploration found multiple whitish granulations disseminated in the entire liver. Biopsy of hepatic granulations made the diagnosis of hepatic tuberculosis. The evolution of anti-tuberculosis medication for nine months was progressive and favorable towards recovery.
Keywords: hepatic granulomatosis; laparoscopy; caseous necrosis
1. Introduction
Hepatic
tuberculosis is a specific infectious pathology corresponding to the
localization in the liver of the koch bacillus (mycobacterium tuberculosis),
which is an alcohol-acid-fast bacillus (afb). Primary hepatic damage is rare
during tuberculosis disease and is usually part of a multivisceral disorder1. The most frequently observed form is the
nodular form2. These nodules can be
large (macronodular tuberculosis) or small (micronodular form) producing the
miliary form of liver tuberculosis found in 80% of cases2. Most patients present with atypical symptoms
that have lasted for a month to a year, such as abdominal pain, weight loss,
generalized weight loss, anorexia, fever, diarrhea, and hepatomegaly on
physical examination3,4. Additional
examinations using abdominal ultrasound, computed tomography (ct) and magnetic
resonance imaging (mri) are non-specific and little contributory4-6. The definitive diagnosis is histological or
bacteriological carried out by ultrasound-guided or scan-guided liver biopsy
which will show an epithelial-gigantocellular granuloma with caseous necrosis7. The treatment is very well codified with a
good prognosis8. We report here the
case of a 38-year-old single housewife who was operated on for cholecystitis
followed by the appearance of cervical adp, in whom the pathological
examination of liver and lymph node biopsies carried out respectively during a
cholecystectomy and puncture trans parietal was able to obtain diagnostic
certainty. The evolution under antibacillary treatment was progressively
towards recovery.
2. Patient and observation
2.1 Patient
information
A young
woman aged 38, single, unemployed, with a history of moderate psychological
deficiency since childhood secondary to neonatal meningitis under no treatment,
consulted for isolated abdominal pain without progressive febrile or icteric
syndrome. For a month, not improved by symptomatic treatments.
2.2 Clinical
results
On
physical examination, there was painful guarding upon palpation of the right
hypochondrium, positive murphy's sign, a temperature of 37.2°c.
2.3 Diagnostic
approach
The biological assessment showed an elevation of crp to 48 mg/l. There was no hyperleukocytosis or anemia, cholestasis or cytolysis, hepatitis b, hepatitis c and hiv serologies were negative. The abdominal ultrasound performed revealed a thin-walled vesicle containing several mini-stones (figure 1).
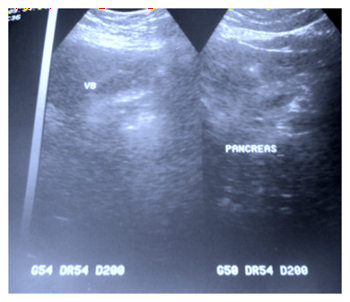
Figure 1. Abdominal ultrasound showing a
vesicle with small stones.
Abdominal
ct scan before (figure 2), and with
opacification confirmed this cholecystitis with a heterogeneous liver with
multiple rounded hypodense microlesions, slightly enhanced after injection of
contrast product (figure 3 images a and
b). A laparoscopy was carried out, where the exploration found multiple
whitish granulations scattered throughout the liver, the rest of the
exploration was unremarkable (figure 4
images a and b).

Figure 2. Abdominal scan in sagittal section without injection of the product showing hypodense formations
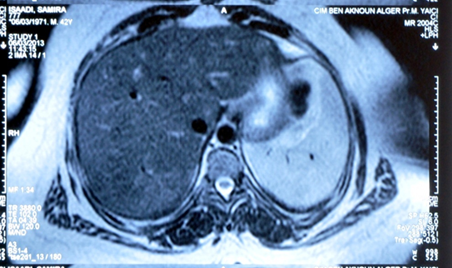

Figure 3. Abdominal scan after injection of contrast product in axial section showing contrast enhancement of liver nodules.
.

Figure 4. Images a and b showing whitish granulations in the liver during
laparoscopy
|
A
cholecystectomy associated with a liver biopsy containing a whitish granulation
was performed (figure 5). The
histological examination of the surgical specimen is that of chronic
cholecystitis in acute post-lithiasic attack, while that of the liver biopsy
showed a hepatic parenchyma site of a moderate steatotic overload with the
presence of 03 gigantocellular epithelial follicles without caseous necrosis.
The
etiological investigation of hepatic granulomatosis including: the metabolic,
autoimmunity and infectious assessments were normal (anti-hcv antibodies,
anti-mitochondria m2 antibodies, protein electrophoresis, enzyme conversion
assay). Pulmonary, upper and lower digestive endoscopy (oesogastroduodenal
fibroscopy, ileocolonoscopy) were without notable features. However, the
intradermal reaction to tuberculin was positive (phlyctenular) at 12mm. The
search for bk by direct examination and culture on biopsies and gastric fluids
was negative.
Abdominal
mri showed isointense t1-t2 hepatic micronodules suggestive of tuberculosis,
sarcoidosis, or other after-effects. One month after the operation, bilateral
oval, hard and painless cervical lymphadenopathy appeared, the cyto-puncture of
which confirmed the nature tuberculosis of hepatic granulations.
1.1
Therapeutic intervention and follow-up The
patient was put on anti-tuberculosis treatment based on her weight for nine
months, combining isoniazid 5 mg/kg, rifampicin 10 mg/kg, ethambutol 25 mg/kg
and pyrazinamide 30 mg/kg for two months and isoniazid with rifampicin for
seven months with monthly clinical and biological monitoring. The evolution was
favorable with apyrexia, weight gain, disappearance of the inflammatory
syndrome after a few weeks, followed by that of lymphadenopathy and hepatic
nodules.
2.
Discussion Hepatic
tuberculosis is often encountered in the context of multi-visceral involvement,
rarely in isolated form, especially in immunocompetent patients1,2. It poses a real diagnostic problem even in
endemic areas because of its nonspecific appearance of its clinical, biological
and radiological signs3. It usually
associates fever, general deterioration, weight loss, sometimes hepatomegaly
with or without jaundice5,6. In our
patient the discovery was fortuitous.
Biologically,
the inflammatory syndrome is present in 50% of cases and can be associated with
anicteric cholestasis in 29% of cases7.
Tuberculin reactions are often positive. The detection of bk on biopsies by
direct examination or by culture is positive in 50% of cases8,9 whereas the amplification of bk by pcr in
samples of hepatic tuberculosis is not still described in the literature. In
our case the inflammatory syndrome is associated only with a strongly positive
tuberculin reaction.
The
contribution of imaging is interesting, but not very specific, and the
micronodular form or miliary hepatic (small hypo-echoic, hypodense nodules with
and without contrast enhancement) is the most common radiological form10,11. On ultrasound, nodules are not always
visualized. In our observation, the lesions were hardly comparable to those
described in the literature.
The
histology is centered by the presence of epithelioid and gigantocellular
granulomas, the appearance of which is not specific. Caseification is present
in almost all cases12,13. In our
patient caseation is absent and the epithelio-gigantocellular follicles are
bathed in a steatotic parenchyma.
The
diagnosis is therefore histological and/or bacteriological, moreover it is
often made on the coexistence of hepatic granulomatosis with another suggestive
localization, in particular pulmonary14,15.
This is the one we encountered, but the suggestive localization was lymph node
and not pulmonary. Finally, the existence of isolated granulomatous hepatitis,
in particular if there are general manifestations, can lead to a trial
treatment which confirms the diagnosis. According to the who recommendations,
the treatment of extrapulmonary localizations without damage to the central
nervous system is based on quadruple anti-tuberculosis therapy for 02 months,
followed by dual therapy for 04 months, the use of which encourages particular
vigilance in the context of biological hepatic disturbance16,17.
3.
Conclusion Primary
hepatic tuberculosis is a rare disease, usually presents in the form of
granulomatous hepatitis, its identification is difficult, even in endemic
areas. The imaging data are not specific, a comparison with epidemiological and
clinico-biological data is necessary. But only the use of puncture-biopsy of
hepatic granulomas carried out during laparoscopy or by guided transparietal
puncture with anatomopathological examination confirms the positive diagnosis.
4.
Conflict of interest None
declared. 5.
Author contributions All
authors approved the final version of the manuscript.
References 1.
Pelletier g. Hepatic tuberculosis.
Hepato-gastro-oncologie digestive 1998;5(6):409. 2.
Nassar i, errabih i, bouklata s, et al.
Primary hepatic tuberculosis: about ten cases. Radiol j 2008;48(4):203-207. 3.
Wang e, sohoni a.
Tuberculosis: a primer for the emergency physician. Em med report 2006. 4.
Tahiri m, goh kl, abbas z, et al.
Tuberculose digestive. World gastroenterology organisation global guidelines.
2021. 8. Kouame n, akaffou e, konan a,
n’goan-domoua a. Miliary hepatitis: a rare ultrasound presentation of hepatic
tuberculosis discovered in an immunocompetent adolescent. Pan afr med j
2011;9(1). 9.
Benhamou jp, bircher j, mcintyre n, et al. Hépatologie
clinique.2002. 12.
Cherki s, adham m, baulieux j, boibieux a,
cotte e. Hepatic tuberculosis. Biol clin gastroenterol 2006;30(11):1317-1320. 16.
Bouvet e, abiteboul d, antoun f, bessa z,
billy c, dautzenberg b. Prevention and treatment of tuberculosis in france.
Summary and recommendations of the group. The quarterly documents for the
occupational physician.2004;(972003):55-64. |