Is Schizophrenia Influenced by Childhood Trauma - A Review Article
ABSTRACT
Keywords: Schizophrenia; Childhood trauma; Adverse childhood experience; Schizotypal personality disorder
INTRODUCTION
About 1% of people suffer from schizophrenia (SCZ), a serious neuropsychiatric illness1 and 20 million people worldwide suffer from the same. Positive, negative, and cognitive symptoms are frequently found in SCZ cases. Positive symptoms align well with auditory hallucinations and mental disorders. Both psychological and cognitive symptoms are present, including learning and concentration problems as well as social disengagement and flat affect in the negative symptoms2. It has been suggested that defective genes and environmental variables interact to cause the symptoms of schizophrenia, which is considered a neurodevelopmental illness. According to the dopamine hypothesis, the hyperfunction of dopamine D2 receptor neurotransmission in the limbic and subcortical brain regions is linked to positive symptoms. Neurotransmission from the D1 receptor is hypoactive, which adds to the negative and cognitive symptoms of schizophrenia3. There are beliefs about the involvement of various natural environmental elements in the development of SCZ, despite the fact that the incidence of SCZ is higher in family members of affected persons. Because multiple exposures are involved, the neurodevelopmental hypothesis of schizophrenia supports the idea that the cause of schizophrenia is a combination of hereditary features and environmental exposures that occur during development, starting in infancy and continuing into adolescence4. Although twin studies found a heritability of about 60-80% for schizophrenia5. According to the two-hit model, a neurodevelopmental issue in the perinatal stage may result in neural circuit failure and stress sensitivity at critical brain times; later, the disorder may be triggered by psychosocial stress or substance misuse, for example6. In addition, when exposed to stresses such as increased alertness and anxiety, schizophrenia patients react emotionally more strongly than non-psychiatric controls7.
Childhood adversity, or childhood trauma (ChT), is the term used to describe traumatic life events including physical, sexual, or emotional abuse or neglect. Adverse childhood experiences (ACEs) are defined as long-term exposure to environmental stressors during early developmental stages. These include living in a household where there is continuing substance misuse, experiencing interpersonal loss, and being mistreated as a youngster. Experiencing parental death, divorce, or mental illness before the age of 17 is considered interpersonal loss8-10. A growing array of literature connects ChT to inflammation, suggesting that inflammation may play a role in the pathophysiology of trauma-related psychopathology10. Those who eventually develop schizophrenia have earlier cognitive deficits in childhood, even though psychotic symptoms usually start in the 18–25 age range. This suggests that cognitive deficiencies are a sign of aberrant neurodevelopment, especially when early developmental adversity is taken into account11. The primary stress neuroendocrine system in the body, the hypothalamus-pituitary-adrenal (HPA) axis, is dysregulated as a neurobiological result of stress sensitization. The HPA axis is involved in the adrenal glands' synthesis of the stress hormone cortisol 12. Stress-induced HPA axis activity heightens stress-induced striatal dopamine release and mesolimbic regions' dopamine sensitization13.
To predict and eventually decrease the development of these disorders in adulthood, it is necessary to first determine the impact that adverse life events experienced during childhood play in psychotic disorders. Though there are various factors about the development of schizophrenia childhood trauma is found to be an important factor for the development as well as affecting the disease progression and treatment rates. However, this is often neglected during assessment and in prevention. Hence this research focuses on the relationship between childhood trauma and schizophrenia.
The purpose of this review is to provide an overview of the role that ChT plays in the onset of schizophrenia and to go into further depth about this idea.
Pathophysiology of Schizophrenia
The pathophysiology of schizophrenia is primarily driven by anomalies in neurotransmitters, including glutamate, gamma-aminobutyric acid (GABA), dopamine, and serotonin. The finding that dopamine D2 receptor blockers effectively reduced psychotic symptoms led to the inadvertent discovery of the relationship between dopamine and schizophrenia14. It is thought that there is an excess of dopamine in the mesolimbic pathway, which links the limbic regions to the ventral tegmental area. This could contribute to the positive symptoms of schizophrenia. Decreased dopamine levels in the mesocortical pathway, which links the cortex and ventral tegmental area, may be the source of negative symptoms and cognitive deficits. Different pathophysiological mechanisms underlie the positive and negative symptoms of schizophrenia, according to these studies. Moreover, the nigrostriatal pathway is tied to extrapyramidal motor side effects brought on by D2 receptor blockers, whereas the tuberoinfundibular pathway is linked to the hyperprolactinemia observed with D2 receptor blocker treatment15. The interaction of glutamate, GABA, and dopamine is essential for controlling the activity of both excitatory and inhibitory interneurons in cortical circuits. Studies conducted after death reveal that schizophrenia is associated with changes in the microstructure and functionality of these microcircuits. These results have led investigators to investigate the possibility of focusing not just on the dopaminergic pathway but also on the glutamate and GABA signalling pathways for more potent therapeutic approaches in schizophrenia16. The schematic representation of the pathophysiology of schizophrenia is shown in (Figure 1)17.
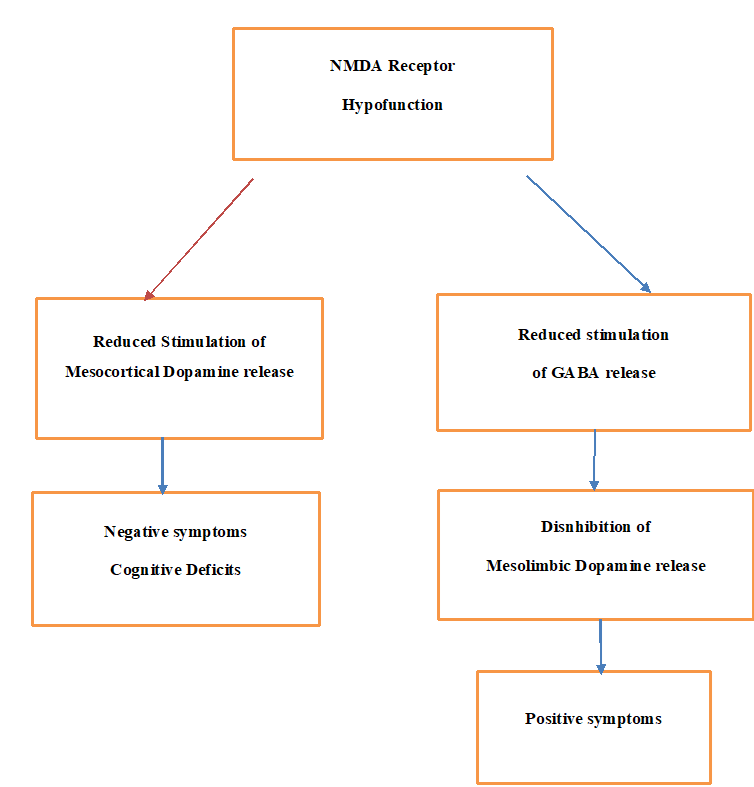
Figure 1. The schematic representation of the pathophysiology of schizophrenia
Genomics of
Schizophrenia
Although
schizophrenia has been better described as an underpinning multifactorial
aetiology with a complex polygenic genetic architecture, genetic epidemiology
investigations have demonstrated that schizophrenia is substantially heritable.
Evidence has been presented in favour of the involvement of several
environmental factors that may contribute to the aetiology of schizophrenia, as
well as frequent and unusual genetic variations linked to the development of
the disorder18. while
more than 100 genetic risk loci for schizophrenia have been found by recent
genome-wide association studies (GWAS), their total contribution to the risk of
schizophrenia is minimal. Furthermore, it has been proposed that the polygenic
risk score could help identify the relationship between intermediate
phenotypes, like the structural changes in the brain that occur in
schizophrenic individuals, and schizophrenia. Furthermore, five CNV areas
associated with schizophrenia have been revealed to contain genes that were
found to express differently in schizophrenia, according to a recent systematic
review of research using copy number variants (CNVs). With a 25-fold increase
in the chance of developing schizophrenia, the 22q11.2 deletion syndrome is the
most thoroughly studied CNV linked to an elevated risk of schizophrenia19 and people with SCZ also have higher
peripheral FKBP5 expression.
However, beyond genetic susceptibility, epigenetics also plays a crucial role
in the development of schizophrenia. The interaction of genetic and
environmental factors during the foetal to developmental stages can potentially
impact and alter the psychopathological course of the illness. Additionally,
other post-developmental factors may influence the onset of schizophrenia
through an epigenetic mechanism. These factors are known as epigenetic factors20,21.
Aspects of Trauma in Childhood
The
capability of a caregiver to provide a safe and healthy environment is directly
proportional to the quality of a child's attachment style. A child's
relationship with the caregiver plays a vital role in early attachment style
formation. Children with responsive caregivers develop secure attachments and
are more open to seeking support when faced with difficulties. On the other
hand, children with unreliable caregivers who fail to care for their needs tend
to develop an avoidant and resistant attachment style, learning to be
emotionally self-reliant at an early age. Childhood exposure to violence can
have negative long-term effects on one's emotional, physical, and mental
well-being. The different ways of childhood trauma are depicted in (Figure 2)22.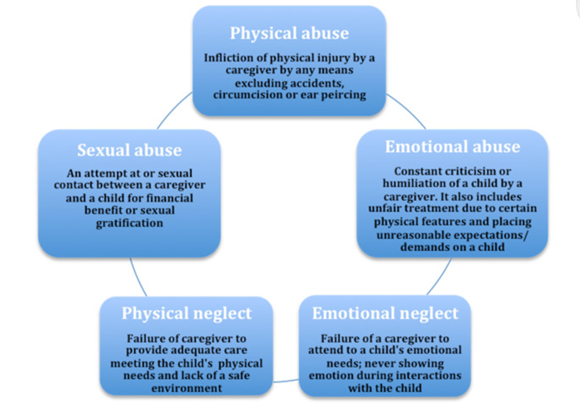
Figure 2. The
different ways of childhood trauma
DISCUSSION
Though
various theories have been postulated for the pathophysiology of schizophrenia
there is a gap in the literature regarding the environmental effects on the
developing brain which leads to the disease. Differential clinical
presentations of schizophrenia spectrum disorders have been linked to several
environmental factors, including childhood adversity, substance use and abuse,
minority and ethnicity status, birth season, urbanity, and pregnancy and perinatal
problems23.
Childhood Trauma and its Effect on the Developing Brain
Severe stress, or ChT,
can leave people in susceptible mental states and increase their risk of
developing mental health conditions like SCZ. Numerous studies show that ACEs
increase the likelihood of psychosis and SCZ development. Higher levels of ChT
cause more heightened positive, general, and depressed symptoms as well as
worse global functioning in ultra-high-risk (UHR) persons. Individuals at UHR
frequently have histories of emotional abuse, physical abuse, emotional
neglect, and sexual abuse24. Findings
were found in a recent South African study investigating the connection between
childhood trauma and SCZ. One physical or emotional trauma experience did not
significantly correlate with schizophrenia. However, those who experienced more
than two of these traumas had a higher chance of developing schizophrenia,
indicating that, even in rare cases, physical and emotional childhood adversity
does not always raise the risk of schizophrenia. However, the likelihood and
intensity of sexual assault increase after just one incident25.
Relationship between Childhood Trauma and Schizophrenia in
Genetic Approach
A gene called FKBP5 is
connected to the hypothalamic-pituitary-adrenal (HPA) axis' stress response.
Notably, the FKBP5 gene plays a role in the development of SCZ when subjected
to acute or prolonged stress. Increased cortisol secretion in ChT-positive schizophrenic
patients points to a link between ChT and the dysfunction of the HPA axis in
SCZ26. In addition to the interaction between genes and
environmental factors, specifically ChT, studies have also shown a direct
correlation between symptoms of schizophrenia-type disorder (SCZ) and the
genetic component brain-derived neurotrophic factor (BDNF) Val66Met
polymorphism. A typical observation in SCZ is the loss of volume in brain
regions such as the hippocampus. When glucocorticoids are used as a stress inducer
in animal models, there is a reduction in hippocampal BDNF levels after both
acute and long-term stress. When used in medical treatments, cortisol can
exacerbate symptoms. SCZ patients exhibit a flattened reactivity to stress and
lower thresholds than controls during and after stress exposure, supporting
that SCZ patients have a significant impairment in their stress response. It's
interesting to note that teenagers who are very susceptible to SCZ have
elevated cortisol levels at rest, which can be attributed to environmental
factors such as emotional abuse from family members and a poor self-image27,28.
Chemical Changes with
Childhood Trauma
ChT
always exhibits modification on the HPA axis. People who have experienced
maltreatment as children have hyperactivity of the axis, which changes dopamine
levels, the autonomic nervous system, the shape of the brain, and neural
function, all of which raise the risk of developing psychosis. Individuals who
experienced childhood hardship showed increased striatal dopamine function,
suggesting a link between associative striatum elevation and psychogenic
stress, particularly physical and sexual abuse29. As
previously mentioned, the primary theory about the pathogenesis of SCZ is that
dopamine overstimulates the brain's D2 receptors. Research suggests that one
important aspect of SCZ is stress sensitization, which lowers the sensitivity
threshold in SCZ patients. Stress can trigger the HPA axis, which makes
dopamine in the mesolimbic area more sensitive and increases dopamine release
in the striatum30.
Brain
Anatomical and Physiological Links to Childhood Trauma
In schizophrenia patients,
emotional neglect was inversely correlated with grey matter volume overall and,
more especially, with the volume and density of the dorsolateral prefrontal
cortex, which was predictive of disorganization. It's interesting to note that
in cases of schizophrenia, there have been reports of additive effects of
childhood trauma and being a BDNF met carrier on volume reduction in the
hippocampal subregions of CA2/3 and CA4/dentate gyrus. Abuse in childhood has
been linked to both decreased hippocampus volume and elevated amygdala
reactivity31. Childhood
trauma was linked to activity of the dorsomedial prefrontal cortex, precuneus,
and posterior cingulate gyrus in patients with schizophrenia during a
theory-of-mind task that mirrored social cognition. Furthermore, patients who
experienced significant degrees of physical and/or sexual abuse as children
have reduced connections between the amygdala and the posterior
cingulate/precuneus region32.
CONCLUSIONS
This review expands on the research that is
currently accessible by recognizing the potential for hardship experienced
throughout childhood and adolescence to manifest into adulthood. However, a
resilience-promoting environment-that is, an environment that integrates
interventions to increase a positive outcome, despite adversities, to implement
wellbeing-is frequently absent from many mental health services, despite the
recovery-oriented approach that is necessary for the management of
schizophrenic patients.
In recent times, acknowledging personal life
experiences has demonstrated advantageous effects on the treatment of many
mental illnesses. The main goal of this study is to highlight how crucial it is
to assess patients holistically, taking into account the impact of their past
experiences on the emergence of present symptoms. Research points to the
brain's neurobiological reactions to trauma as a risk factor for SCZ
development. To demonstrate the realistic potential of neurological effect
regulation, it will be imperative in further trials to assess the advantages of
early trauma detection and the accessibility of early support. Finding a
beneficial effect on neurobiology ought to motivate additional primary care
physicians to include early trauma screening in child wellbeing visits. In a
perfect world, early identification of adversity in individuals would result in
the prompt introduction of resources that help address mental and emotional
dysregulations; this might be a crucial step in reducing the annual diagnostic
rate and severity of schizophrenia in the general population.
Author
Contributions: My
co-authors' contributions to the creation of this review are greatly
appreciated. I sincerely thank everyone who contributed equally to the creation
of this review. Zareen Zohara and Ajeeth Rehman Abdul Jaffar Azad. Conceptualized
the Project: Ajeeth Rehman Abdul Jaffar Azad handled the methodology; Faizal
Khan. Handled the software: Zareen Zohara and Ajeeth Rehman Abdul Jaffar Azad
validated the work; Zareen Zohara conducted the formal analysis; Zareen Zohara,
Faizal Khan, and Ajeeth Rehman Abdul Jaffar Azad conducted the investigation;
Zareen Zohara and Ajeeth Rehman Abdul Jaffar Azad handled the resources; Zareen
Zohara and Ajeeth Rehman Abdul Jaffar Azad prepared the data; Zareen Zohara
prepared the original draft; Ajeeth Rehman Abdul Jaffar Azad handled the
writing; Zareen Zohara and Ajeeth Rehman Abdul Jaffar Azad handled the review
and editing; Zareen Zohara. Zohara Zareen. Each author has reviewed the
published version of the manuscript and given their approval.
Funding: There is no funding to declare
Acknowledgements:
In this section, you can acknowledge any support given which is not covered by
the author contribution or funding sections. This may include administrative
and technical support, or donations in kind (e.g., materials used for
experiments).
Conflicts of Interest:
The authors declare no conflict of interest.
REFERENCES
2. Stępnicki P, Kondej M, Kaczor AA.
Current concepts and treatments of schizophrenia. Molecules 2018;23(8):2087.
3. Syed AB, Brasic JR. The role of lumateperone in the
treatment of schizophrenia. Ther
Adv Psychopharmacol 2021;11.
4. Kesby JP, Eyles DW, McGrath JJ, Scott
JG. Dopamine, psychosis and schizophrenia: the widening gap between basic and
clinical neuroscience. Transl
Psychiatry 2018;8:30.
5. Sullivan PF, Kendler KS, Neale MC. Schizophrenia as
a complex trait: evidence from a meta-analysis of twin studies. Arch Gen Psychiatry 2003;60(12):1187-1192.
6. Schmitt A, Malchow B, Hasan A. Falkai P. The impact
of environmental factors in severe psychiatric disorders. Front Neurosci 2014;8:19.
7. Docherty NM, St-Hilaire A, Aakre JM, Seghers JP.
Life events and high-trait reactivity together predict psychotic symptom
increases in schizophrenia. Schizophr Bull 2009;35(3):638-645.
8. Bhavsar V, Boydell J, McGuire P,
et al. Childhood abuse and psychotic experiences - evidence for mediation by
adulthood adverse life events. Epidemiol
Psychiatr Sci 2019;28:300-309.
9. Beal SJ, Wingrove T, Mara CA,
Lutz N, Noll JG, Greiner MV. Childhood adversity and associated psychosocial
function in adolescents with complex trauma. Child Youth Care Forum 2019;48(3):305-322.
10. Devi F, Shahwan S, Teh WL,
et al. The prevalence of childhood trauma in psychiatric outpatients. Ann Gen Psychiatry 2019;18:15.
11. Sheffield JM, Karcher NR, Barch DM. Cognitive
deficits in psychotic disorders: a lifespan perspective. Neuropsychol Rev 2018;28(4):509-533.
12. Holtzman CW, Trotman HD, Goulding
SM, et al. Stress and neurodevelopmental processes in the emergence of
psychosis. Neuroscience 2013;
249:172-191.
13. van Winkel R, Stefanis NC,
Myin-Germeys I. Psychosocial stress and psychosis.A review of the
neurobiological mechanisms and the evidence for gene-stress interaction. Schizophr
Bull 2008;34:1095-1105.
14. Marder SR, Cannon TD.
Schizophrenia. N Engl J Med 2019;381(18):1753-1761.
15. Robison AJ, Thakkar KN, Diwadkar
VA. Cognition and Reward Circuits in Schizophrenia: Synergistic, Not
Separate. Biol Psychiatry 2020;87(3):204-214.
16. Lavretsky H.
History of Schizophrenia as a Psychiatric Disorder. In: Clinical Handbook of Schizophrenia. New
York, Guilford Press 2008;3-12.
17. Dawe GS, Hwang EH, Tan CH.
Pathophysiology and animal models of schizophrenia. Ann Acad Med Singapore 2009;38(5):425-426.
18. Owen MJ, Sawa A, Mortensen PB.
Schizophrenia. Lancet Lond. Engl 2016;388:86-97.
19. Merikangas
AK, Shelly M, Knighton A, et al. What Genes Are Differentially Expressed in
Individuals with Schizophrenia? A Systematic Review. Mol. Psychiatry 2022;27:1373-1383.
20. Radua J,
Ramella-Cravaro V, Ioannidis JPA, et al. What Causes Psychosis? An Umbrella
Review of Risk and Protective Factors. World Psychiatry 2018;17(1):49-66.
21. Smigielski L, Jagannath V, Rossler
W, Waltiza S, Grunblatt E. Epigenetic mechanisms in schizophrenia and other
psychotic disorders: A systematic review of empirical human findings. Mol. Psychiatry 2020;25(8):1718-1748.
22. Zeanah CH, Humphreys KL. Child abuse
and neglect. J Am Acad Child Adolesc Psychiatry 2018;57:637-644.
23. Pence AY,
Pries LK, Ferrara M, et al. Gender Differences in the Association between
Environment and Psychosis. Schizophr.
Res 2022;243:120-137.
24. Popovic D,
Schmitt A, Kaurani L, et al. Childhood trauma in schizophrenia: current
findings and research perspectives. Front
Neurosci 2019;13:274.
25. Sallis HM,
Croft J, Havdahl A, et al. Genetic liability to schizophrenia is
associated with exposure to traumatic events in childhood. Psychol Med 2021;51(11):1814-1821.
26. Stramecki
F, Misiak B, Frydecka D. The role of the interaction between the fkbp5
gene and stressful life events in the pathophysiology of schizophrenia: A
narrative review. Arch Psychiatry
Psychother 2020;3:7-16.
27. Bi XJ, Lv
XM, Ai XY, et al. Childhood trauma interacted with BDNF Val66Met influence
schizophrenic symptoms. Medicine (Baltimore) 2018;97(13):0160.
28. Kauppi K, Westlye LT, Tesli M, et
al. Polygenic Risk for Schizophrenia Associated with Working Memory-Related
Prefrontal Brain Activation in Patients with Schizophrenia and Healthy Controls. Schizophr Bull 2015;41(3):736-743.
29. Egerton A,
Valmaggia LR, Howes OD, et al. Adversity in childhood linked to elevated
striatal dopamine function in adulthood. Schizophr
Res 2016;176(2):171-176.
30. Gabínio T,
Ricci T, Kahn JP, et al. Early trauma, attachment experiences and comorbidities
in schizophrenia. Trends Psychiatry
Psychothe 2018;40:179-184.
31. Aas M, Haukvik UK, Djurovic S, et
al. Interplay between childhood trauma and BDNF val66met variants on blood BDNF
mRNA levels and hippocampus subfields volumes in schizophrenia spectrum and
bipolar disorders . J Psychiatr Res 2014;59:14-21.
32. Quide Y,Ong XH, Mohnke S, et al.
Childhood trauma-related alterations in brain function during a Theory-of-Mind
task in schizophrenia. Schizophr Res 2017;189:162-168.