Laryngeal Lipoma: A Rare Diagnosis of Submucosal Mass with Progressive Dysphonia
Abstract
Laryngeal lipomas are rare benign tumors, accounting for less than 1%
of benign neoplasms in this region. This report describes the case of a
60-year-old patient with progressive dysphonia, choking episodes, and chronic
throat clearing, in whom videolaryngoscopy and computed tomography identified a
submucosal mass in the larynx. The patient underwent surgical excision via
lateral cervicotomy, and histopathological analysis revealed a spindle cell
lipoma, an uncommon variant with myxoid matrix and positive CD34 expression.
The postoperative course was satisfactory, with no signs of recurrence after
three months. This case highlights the importance of early differential
diagnosis of laryngeal masses and the role of complete excision in achieving a
favorable prognosis. Case documentation contributes to improved recognition and
management of rare laryngeal tumors.
Keywords: Immunohistochemical; Lipoma; Larynx; Rare; Surgical
Introduction
Laryngeal tumors are mostly malignant, with squamous cell carcinoma
being the most common type. However, benign tumors can also occur, although
significantly less frequently1,2. Among these, laryngeal lipoma stands out as a
rare entity, with few cases reported in the literature. Lipoma is a mesenchymal
tumor composed of mature adipose tissue and is one of the most common benign
tumors in the human body. When located in the larynx, its occurrence is
extremely rare, accounting for less than 1% of all benign tumors in this
region3. The etiology of laryngeal lipoma remains uncertain, and clinical
manifestations depend on the tumor’s size and precise location. Generally,
lipomas are asymptomatic and slow-growing, but in the larynx, they may cause
significant symptoms due to airway obstruction or compression of adjacent
anatomical structures. Common symptoms include hoarseness, respiratory
difficulty, and dysphagia, often mistaken for more prevalent conditions such as
laryngeal polyps or cysts4. Due to its rarity, early and accurate diagnosis of
laryngeal lipoma can be challenging and is frequently confused with other
benign or malignant laryngeal masses5.
Objectives
This report aims to describe a clinical case of a 60-year-old patient
with a submucosal laryngeal mass and progressive dysphonia.
Materials and Methods
A retrospective case report was conducted through electronic medical
record review, accompanied by a brief literature review.
Case Report
A 60-year-old male patient sought otolaryngologic care due to chronic
coughing, throat clearing, and hoarseness, with progressive worsening of
dysphonia in recent months6. With a history of thyroidectomy five years earlier
and on levothyroxine (Puran), he underwent videolaryngoscopy, which revealed a
cystic submucosal lesion in the vallecula and left laryngeal wall, with glottic
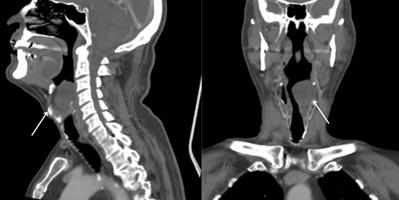
compression. A computed tomography scan showed a 3.7 × 3.7 cm heterogeneous
hypodense formation in the left paraglottic region, significantly reducing the
glottic and supraglottic airway column7,8. Referred to Head and Neck Surgery,
the patient underwent lesion resection via lateral cervicotomy.
Histopathological examination revealed a low-grade myxoid mesenchymal neoplasm,
consistent with spindle cell lipoma, characterized by abundant myxoid matrix,
elongated paucicellular cells, absence of atypia, and positive CD34
immunohistochemical staining9. Postoperatively, the patient recovered well, was
discharged the same day with prophylactic antibiotics, and advised to return in
three months with a new imaging exam10. At outpatient follow-up, he presented
asymptomatic with no signs of recurrence and a favourable clinical prognosis
(Figure 1).
Figure 1: Computed tomography of the neck, showing a hypodense formation in the fat of the left paraglottic space measuring 3.7 x 3.7 cm, causing local bulging with reduction of the airway column in the glottic and supraglottic larynx
Conclusion
Although rare, the spindle cell variant of laryngeal lipoma has an
excellent outcome when correctly diagnosed. Meticulous histopathological
distinction from other mesenchymal neoplasms avoids inadequate treatment and
reduces the risk of recurrence. Wide surgical excision remains the gold
standard therapy, restoring airway patency and vocal function with minimal
morbidity. Periodic follow-up with laryngoscopy is essential for early
detection of recurrence. The expansion of clinical case reports will aid in greater
recognition and refinement of diagnostic and management protocols for this
uncommon entity.
References
1. Gross M. et al.
Laryngeal lipoma: a rare cause of airway obstruction. Otolaryngology-Head and
Neck Surg 2005;132(3):505-506.
2. Chuang HC, et al.
Spindle cell lipoma of the larynx. J Clin Pathology 2006;59(8):888-890.
3. Enzinger FM, Weiss SW.
Soft Tissue Tumors. 5. ed. St. Louis: Mosby 2008.
4. Pereira JC, et al.
Lipoma laríngeo: apresentação incomum de massa submucosa. Revista Brasileira de
Otorrinolaringologia 2008;74(5):785-789.
5. Ferreira LV, et al.
Tumores benignos da laringe: análise de 100 casos. Arquivos Internacionais de
Otorrinolaringologia 2008;12(3):356-361.
6. Shukla D. et al.
Spindle cell lipoma in head and neck: A rare diagnosis. Indian Journal of
Pathology and Microbiology, v. 53, n. 1, p. 124-126, 2010.
7. Yang BT, et al. CT and
MR imaging of benign laryngeal tumours. American J Neuroradiology
2010;31(2):262-269.
8. Kolesnikov AI, et al.
Lipomas of the larynx and hypopharynx: diagnosis and treatment. Vestnik
Otorinolaringologii 2014;79(1):43-45.
9. Bouhelier, E. et al.
Cervical approach for resection of large paraglottic space tumours. European
Annals of Otorhinolaryngology, Head and Neck Diseases 2016;133(3):195-198.
10. Morais MS, et al.
Tumores benignos de laringe: revisão de literatura e considerações clínicas.
Revista Brasileira de Cirurgia de Cabeça e Pescoço 2019;48(1):17-22.