Link between Chronic Kidney Disease (CKD) and Known Risk Factors: A Hospital-based Study in Pakistan
Abstract
Background and objective: chronic kidney disease (ckd) is a progressive disease which is not curable with high morbidity and mortality rate. Despite the harmful consequences of ckd, few studies have been conducted in pakistan regarding ckd which are also outdated. So, the objective of the study was to determine the socio-demographic and preventable clinical risk factors associated with ckd.
Methods: patients visiting the outdoor department of nephrology or those admitted in ward between feb-nov 2019 were selected for the study. A questionnaire including demographic information and risk factors for ckd was filled after informed consent. Data was analyzed on spss software. Main outcome measures: risk factors including hypertension, diabetes, positive history of ckd and kidney stone were found to be associated with ckd development.
Results: a total of 200 patients participated in the study in which 131 (65.5%) were female. Risk factor data revealed older age (p-value 0.02), hypertension (p-value 0.02), diabetes (p-value 0.03) and positive family history of ckd (p-value 0.01) to be associated with disease development. Logistic regression revealed that old age increases the odds of ckd by 3 times followed by positive family history of ckd (or: 2.2) and history of renal stone (or: 1.8).
Conclusion: numerous risk factors are associated with the progression of ckd. Our findings are the first to provide a quantitative estimate of the risk posed by different factors on ckd in pakistan. Our findings emphasize the pressing need for designing early detection and treatment plans for ckd followed by its prevention policies in pakistan.
Key words: chronic kidney disease; diabetes; hypertension; kidney disease; risk factors
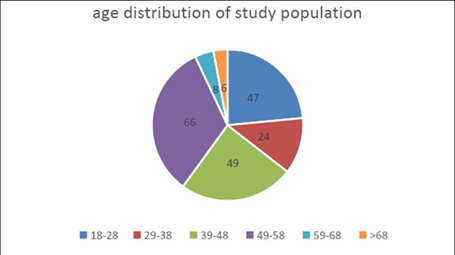
Figure 1. Age distribution of study participants
Data related to the ckd of the patients and history of hypertension, dm and cardiovascular diseases among the patients and adjusted ratio of the factors related to ckd has been shown below.
(table 1) shows information related to
various risk factors of ckd. Majority of the patients in the study were females. Almost all the risk
factors were found in the patients reporting to the renal department with the majority of
the patients already suffering from diabetes and hypertension.
Table 1. Frequency
of risk factors in study participants
|
Variable |
Frequency N
(%) |
|
Sex |
|
|
Female |
131 (65.5) |
|
Male |
69 (34.5) |
|
History of htn |
|
|
No |
49(24.5) |
|
Yes |
151(75.5) |
|
History of dm |
|
|
No |
23(11.5) |
|
Yes |
177(88.5) |
|
History of
cigarette smoking |
|
|
No |
125(62.5) |
|
Yes |
75(37.5) |
|
History of
nsaids |
|
|
No |
30(15) |
|
Yes |
170(85) |
|
History of
ckd in family |
|
|
No |
90(45) |
|
Yes |
110(55) |
|
History of renal
stone |
|
|
No |
179(89.5) |
|
Yes |
21(10.5) |
Htn: hypertension, dm: diabetes mellitus, nsaids: non-steroidal anti-inflammatory drugs, ckd: chronic kidney disease
To confirm if the demographic variables and known environmental factors actually played a significant role in the development of chronic kidney disease (ckd), chi‐square test was performed andp < 0.05 was considered significant (table 2). Results revealed that factors including age between 39-48, history of hypertension, dm, use of drugs and positive history of ckd in family were statistically significant for their role in the development of ckd (table 2).
Table 2. Risk factors for chronic kidney disease
|
Variables |
Frequency of patients (n) |
P-value |
|
Age |
|
|
|
18-28 |
47 |
0.07 |
|
29-38 |
24 |
0.08 |
|
39-48 |
49 |
0.01 |
|
49-58 |
66 |
0.28 |
|
59-68 |
8 |
0.19 |
|
>68 |
6 |
0.02 |
|
History of htn |
|
|
|
No |
49 |
0.02 |
|
Yes |
151 | |
|
History of
dm |
|
|
|
No |
23 |
0.03 |
|
Yes |
177 | |
|
History of
cigarette smoking |
|
|
|
No |
125 |
0.75 |
|
Yes |
75 | |
|
History of
nsaids |
|
|
|
No |
30 |
0.01 |
|
Yes |
170 | |
|
History of ckd in
family |
|
|
|
No |
90 |
0.01 |
|
Yes |
110 | |
|
History of renal
stone |
|
|
|
No |
179 |
0.79 |
|
Yes |
21 |
Htn: hypertension, dm: diabetes mellitus, nsaids: non-steroidal anti-inflammatory drugs, ckd: chronic kidney disease
These factors were further evaluated through logistic regression for calculation of odds ratio (table 3). Old age showed the highest odds of increasing ckd by 3 times followed by positive family history of ckd (or: 2.2) and history of renal stone (or: 1.8).
Table 3. Logistic regression for risk factors of ckd
|
Variables |
Aor (95% ci) |
|
Age |
|
|
18-28 |
1.46(1.05,2.03) |
|
29-38 |
1.50(0.95,2.36) |
|
39-48 |
2.40(1.59,3.65) |
|
49-58 |
0.77(0.49,1.23) |
|
59-68 |
1.40(0.85,2.32) |
|
>68 |
3.16(1.36,7.35) |
|
History of htn |
1.26(0.97,1.64) |
|
History of
dm |
0.70(0.51,0.96) |
|
History of
cigarette smoking |
1.05(0.76,1.45) |
|
History of nsaids |
0.48(0.37,0.61) |
|
History of
ckd in family |
2.22(1.65,2.98) |
|
History of renal
stone |
1.76(1.34,2.31) |
Htn: hypertension, dm: diabetes mellitus, nsaids: non-steroidal anti-inflammatory drugs, ckd: chronic kidney disease
1. Discussion
Chronic kidney disease (ckd)
is a progressive disease which is not curable
with high morbidity and mortality
rate10. Our study is the first to quantify the risk posed by
socio-demographic and preventable
clinical risk factors associated with ckd.
Age
is documented as an independent risk factor for the development of renal disease11 and our
findings of high prevalence of ckd in older people were consistent with
previous studies9,12.
Hypertension and diabetes
are considered strong predictors for kidney dysfunction progression13,14.
We found strong association of htn and dm with ckd in our study which is consistent with previous studies done in
other countries15,16.
Our results are also consistent with findings
from a study done by jessani et al., in 20149. Another important risk factor was
positive family history of ckd. We
found that the odds of ckd increase 2.2 times if the disease is already present in the family. Previous
studies have also demonstrated positive family history as predictors of ckd17. Okwuonu et al., 2017 found that the odds
of ckd increase by 4.5 times in these cases18. This is the first study from pakistan that has provided
a quantitative estimate
of the risk posed by positive family history on the development of
ckd.
Kidney stones have long been associated with elevated risk for chronic renal disease. Our study shows that the risk of ckd increases by almost 1.8 times in patients with a positive history of kidney stones. A study from taiwan19 also found an association between kidney stones and poor ckd prognosis. Two recent studies have also highlighted the strong association between kidney stone and ckd20,21. Hence, it can be said that htn, dm, positive history of ckd and kidney stones are among the major causes of ckd in pakistan.
Smoking
is also associated with cdk. Our results of 1.05 odds ratio are comparable with
an american study done in 2018 which
also showed odds ratio of 1.02 for ckd progression22. However, detailed studies need to be done in this area for comprehensive
results.
The
present study had its limitations that are worth mentioning. Firstly, serum
creatinine level was used for the
diagnosis of ckd in which albuminuria
was not taken into consideration. Diet, total
muscle mass, and comorbidities can affect creatinine levels which can in turn
lead to a misclassification of the
outcome. However, other studies have also used single measurement for epidemiological research23.
Secondly; the study was conducted in lahore so findings can be different in other areas of pakistan.
However, healthcare services provided in other areas are not better than lahore.
We recommend comprehensive studies to be conducted for exact identification of the burden posed by ckd
and controlling its risk factors in different areas of the country
for disease prevention. Only
then, effective policies to control ckd can be formulated.
2. Conclusion
Numerous risk factors are associated with the progression of ckd. Our findings are the first to provide a quantitative estimate of the risk posed by different factors on ckd in pakistan. Our findings emphasize the pressing need for designing early detection and treatment plans for ckd followed by its prevention policies in pakistan, and other developing countries with high ckd burden.
3. Acknowledgement
We would like to express our heartfelt gratitude and appreciation to ayesha bashir hospital pakistan for all the support the center provided during the course of study and special thanks to dr. Ijaz bashir for his expertise and assistance throughout all aspects of the study.
4. Conflicts of interest
None declared
5. Financial support & sponsorship
None received
References
4. Gbd
2015 mortality and causes of death collaborators. Global, regional, and
national life expectancy, all-cause mortality, and cause-specific
mortality for 249 causes of death, 1980-2015: a systematic analysis for
the global burden of disease study 2015. Lancet 2016;388:1459-1544.
5. Garcia-garcia
g, jha v. World kidney day steering committee. Ckd in disadvantaged populations.
Kidney int 2015;87:251-253.
10. Webster ac, nagler
ev, morton rl, masson p. Chronic kidney disease. Lancet
2017;389(10075):1238-1252.
20. Jaime u. Chronic kidney
disease and kidney stones. Curr opin nephrol hypertens 2020;29(2):237-242.