Lipoma of the Parotid Gland Extending from the Superficial to the deep Lobe: Case Report
ABSTRACT
Case Report:
we present in this article a clinical case of a lipoma of the
superficial lobe of the parotid gland
Discussion: The clinical diagnosis of parotid
lipomas is difficult since they are most often asymptomatic or, when
symptomatic, manifest only as a painless swelling of the parotid gland.
Magnetic resonance imaging is the most accurate in preoperative diagnosis. The
diagnosis is confirmed by histological examination. In their surgical
management, parotid lipomas should be considered as any other parotid tumor
since we cannot exclude malignancy. Surgical complete resection should be
performed, with preservation of the facial nerve.
Keywords:
Lipoma; Parotid gland; Superficial parotidectomy; Facial nerve.
INTRODUCTION
Lipoma is one
of the most common mesenchymal soft tissue tumors. Over 10% arise in the head
and neck region, especially in the posterior cervical triangle and forehead1. Only exceptionally do they occur in the oral
cavity, pharynx, larynx, and parotid gland. In this article, we describe a
clinical case of superficial lobe parotid lipoma, and discuss the different
diagnostic and therapeutic modalities.
CASE REPORT
A 47-year-old woman, with no medical past history, was
referred to our department for a right preauricular swelling that had been
slowly growing for 1 year. The patient had not experienced pain or any other
symptoms (Figure 1).
Clinical
examination revealed an obviously visible mass located in the region of the
right parotid gland near the angle of the mandible, mobile, well-circumscribed,
measuring 3 cm, with a firm consistency and no inflammatory signs or skin
changes overlying it. There were no associated lymph nodes. No signs of
peripheral facial nerve palsy were identified. The patient was, besides, obese
with a BMI of 41 kg/m². The
rest of the clinical examination didn’t reveal any abnormalities.
Figure 1. Patient’s preoperative view reveals a swelling of the
right parotid gland.
On magnetic
resonance imaging (MRI), a 31x26x30 mm oval-shaped lesion with well-defined
contours was identified in the inferior part of the superficial lobe of the
right parotid gland. It was partially extended to the
deep lobe. The lesion exhibited homogeneity and very high intensity on
T1-weighted images, high intensity on T2-weighted images, and low intensity on
diffusion-weighted images. The lesion was not enhanced after gadolinium
injection. This intensity pattern was identical to that of the fatty tissue (Figure 2).
Therefore,
the images suggested the diagnosis of parotid lipoma.
Under general
anesthesia, superficial parotidectomy with preservation of facial nerve was
performed. Surgery began with a modified Blair’s incision, the parotid gland
was then exposed. After identifying the facial nerve trunk and its
branches, the fatty mass was completely excised together with part of the
adjacent superficial lobe from which it was originating (Figure 3).

Figure 2. MRI images
show the fatty mass in the right parotid gland.
During
surgery, frozen section was sent to decide further course of action. Gross
examination of the specimen sent disclosed a mass of adipose tissue measuring
4,5x 3,3 x1,1 cm surrounded by salivary gland tissue. Thus, the frozen section
examination reported that the mass is likely a parotid lipoma, negative for
malignancy.
A redon drain
was inserted for 48 hours, and the wound was closed in layers. The patient
sustained no postoperative complications.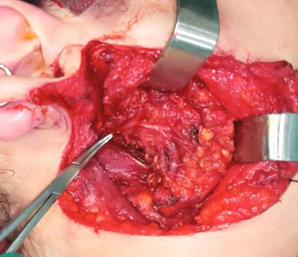

Figure 3. Intraoperative view after
superficial parotidectomy with preservation of the facial nerve.
A
postoperative detailed histopathological examination of the resected specimen
confirmed that the mass was indeed a parotid lipoma.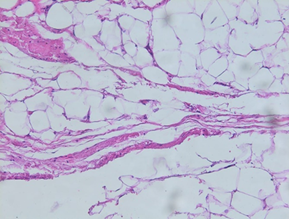
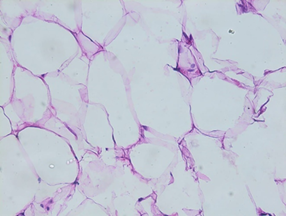
Figure 4. Histological section of parotid
gland lipoma.
Figure
5. Patient’s
postoperative photos show a normal facial nerve function.
DISCUSSION
Although
lipomas are the most frequently occurring soft tissue mesenchymal tumors,
their location in the parotid gland is quite uncommon with a range of 0.6 to 4%
of all parotid gland masses2-4. Very
few parotid lipomas have been reported in the literature and most of them are
single case reports. The largest series to date, to our knowledge, is about 70
cases2.
Lipomas can
be seen in a broad age range from 6 months to 72 years, but they occur mainly
in adults in the fifth to the sixth decade of life, and are less frequent in
the pediatric population2,4-6. The
age range in the largest series is 7.4 to 89.5 years2.
Parotid
lipomas have a predilection to males with a male to female ratio of 3:1 in most
studies2,5. A wider gap (10:1) has
been noted in an older large series4.
The
literature suggests that risk factors of lipomas include heredity, obesity,
diabetes, endocrine disorders, corticosteroid therapy, trauma, and radiation7. The patient in our case was morbidly obese.
Parotid
lipomas occur in equal frequency on the right and left sides and are rarely
found to be bilateral. The majority of them arise from the superficial lobe,
the deep lobe is rarely involved1,8.
Clinical
diagnosis of parotid lipomas is difficult, as they manifest with few symptoms,
especially those originating in the deep lobe. Generally, they appear as
slow-growing asymptomatic masses, soft, well-circumscribed, mobile,
compressible, and painless. their size varies from 1 to 8 cm7,9. They are not known to be associated with
any skin changes or other salivary gland lesions. Besides, neurological
deficits are remarkably rare2,4 with
only one case of facial palsy reported10.
When
diagnosis is based only on clinical findings, parotid lipoma is seldom
considered in the initial differential diagnosis of a parotid mass. The most
commonly reported clinical diagnoses before any imaging are pleomorphic adenoma
and Warthin tumor2,5.
Ultrasonography
(US) is usually the first imaging modality used to explore parotid gland
tumors. Thus, knowledge of the sonographic semiology of lipomatous tumors is
fundamental. Lipomas are typically well-defined elliptical compressible masses,
generally hyperechoic to adjacent muscle with the longest diameter parallel to
the skin surface. They show no evidence of posterior enhancement or attenuation
and no flow on color Doppler sonography. Lipomas have also been described as
hypoechoic or isoechoic. Therefore, ultrasonography is not highly specific11,12.
Computed tomography (CT) is extremely useful
in preoperative diagnosis of parotid lipomas. The classic appearance of lipoma
in CT is a circumscribed homogenous hypodense mass with few septations. Since
fat is the only soft tissue with a density less than water, lipomas show a
characteristic low CT attenuation number ranging from -150 to -50 Hounsfield
Units. This typical fat attenuation enables the diagnosis of
lipoma. Nevertheless, in case of fibrolipoma, a high density may be
observed on the CT scan, due to the increased amount of fibrotic tissue in that
subtype of lipomas13,14. Moreover,
lipomas do not enhance after contrast material
administration except in cases of angiolipomas. CT scan helps also to define
the location and extent of the tumor. However, it does not significantly help
to differentiate the lipoma from the surrounding adipose tissue2,6,8.
Magnetic resonance imaging (MRI) remains the
best diagnostic modality of parotid lipomas. Not only does it enable a more
accurate preoperative diagnosis, but MRI has also proved to be superior to CT
in localizing and defining tumor margins.
Typically, lipomas display
high signal on T1-weighted images, low signal on T2-weighted images and can be
definitively diagnosed as tumors of adipocytic origin on fat-suppressed or STIR
sequences. Furthermore, the margin of a lipoma is distinctly delineated as a "black rim" allowing, thus, to distinguish
lipomas from surrounding adipose tissue2,5,6.
The weakness of imaging as a whole is its
inability to definitively differentiate a lipoma from a liposarcoma. Only
histopathological examination can establish the diagnosis with certainty11.
Fine needle aspiration cytology, which is
considered a relevant tool in the investigations of a parotid mass, has been
described as inaccurate for the diagnosis of parotid lipoma, essentially
because fat cells from lipomas are histologically indistinguishable from normal
subcutaneous fat15,16.
The surgical management of parotid lipomas
requires the same approach as for any other parotid tumor, considering the
existence of the facial nerve in the operative field, and the impossibility to
definitively exclude malignancy. Thus, the aim of surgery is to perform, if
possible, a complete resection of the mass with a margin of normal parotid
tissue, and at the same time preserve the facial nerve.
The surgical technique depends mainly on the
size and location of the lipoma. Most authors recommend superficial
parotidectomy with dissection and preservation of the facial nerve for tumors
located within the superficial lobe.
As for lipomas located in the deep lobe,
total parotidectomy is generally preferred. Most surgeons recommend superficial
parotidectomy with dissection of the facial nerve before removal of lesions in
the deep lobe1 For some tumors, the
superficial lobe can be placed back over the facial nerve after resection of a
deep lobe tumor, in order to prevent neurological deficits.
Enucleation or complete excision with a thin
layer of normal parotid gland parenchyma have been suggested in cases of
encapsulated intra or paraparotid lipomas2. However, superficial parotidectomy is preferred by most investigators.
Although complete surgical excision is the
gold standard for treatment of parotid tumors, the accuracy of the diagnosis
made by imaging modalities in most cases has led some authors to propose
long-term clinical and radiological surveillance as a way to manage small
intraparotid lipomas.
CONCLUSION
Parotid lipoma is a rare benign lesion that
should be considered among the differential diagnoses of a parotid mass.
Appropriate imaging can be very accurate in preoperative diagnosis. Definitive
diagnosis is only accomplished with histopathological review. Complete surgical
excision should be performed meticulously to avoid postoperative facial palsy.
REFERENCES
1. Debnath SC, Saikia A. Lipoma of the parotid gland
extending from the superficial to the deep lobe: a rarity. Br J Oral Maxillofaci
Sur 2010;48(3):203‑204.
2. Starkman SJ, Olsen SM, Lewis JE, Olsen KD, Sabri A.
Lipomatous lesions of the parotid gland: Analysis of 70 cases. Laryngoscope 2013;123(3):651‑656.
3. Baker SE, Jensen JL, Correll RW. Lipomas of the
parotid gland. Oral Sur, Oral Med, Oral Pathol 1981;52(2):167‑171.
4. Walts AE, Perzik SL. Lipomatous lesions of the parotid
area. Arch Otolaryngol 1976;102(4):230‑232.
5. Ethunandan M, Vura G, Umar T, et al. Lipomatous
Lesions of the Parotid Gland. J Oral
Maxillofaci Sur 2006;64(11):1583‑1586.
6. Baykul T, Aydin MA, Findik Y, Yildirım D. Huge lipoma
of the right parotid gland: Case Report and Review of 42 Cases. Ear Nose Throat
J 2016;95(1):8‑13.
7. Tilaveridis I, Kalaitsidou I, Pastelli N, Antoniades
K. Lipoma of parotid gland: Report of two cases. J Maxillofac Oral Surg 2018;17(4):453‑457.
8. El-Monem MHA, Gaafar AH, Magdy EA. Lipomas of the head
and neck: Presentation variability and diagnostic work-up. J Laryngol Otol
2006;120(1):47-55.
9. Furlong MA, Fanburg-Smith JC, Childers ELB. Lipoma of
the oral and maxillofacial region: Site and subclassification of 125 cases.
Oral Sur Oral Med Oral Pathol Oral Radiol Endod 2004;98(4):441‑450.
10. Srinivasan V, Ganesan S, Premachandra DJ. Lipoma of
the parotid gland presenting with facial palsy. J Laryngol Otol 1996;110(1):93‑95.
11. Tong KN, Seltzer S, Castle JT. Lipoma of the parotid
gland. Head neck pathol 2020;14(1):220‑223.
12. Ahuja AT, King AD, Kew J, King W, Metreweli C. Head
and neck lipomas: Sonographic appearance. AJNR Am J Neuroradiol 1998;19(3):505‑508.
13. Saitoh Y, Hama T,
Ishizaka S, et al. Fibrolipoma
of the parotid in a child. Am J Otolaryngol 1995;16(6):433‑435.
14. Choi HJ. Preauricular fibrolipoma presenting as upper
parotid tumor. J Craniofac Sur 2015;26(2):601‑602.
15. Arslan IB, Uluyol S, Genc S, Eruyar T, Bulgurcu S,
Cukurova I. Diagnostic dilemma of parotid lipomas: Imaging versus fine needle
aspiration cytology. Bosn J Basic Med Sci 2014;14(4):250‑253.
16. Layfield LJ, Glasgow BJ, Goldstein N, Lufkin R.
Lipomatous lesions of the parotid gland. Potential pitfalls in fine needle
aspiration biopsy diagnosis. Acta Cytol 1991;35(5):553‑556.