Management of a Piece of Glass Cervical Foreign Body Introduced by Penetrating Trauma: Case Report and Literature Review
Abstract
Cervical penetrating trauma is particularly dangerous,
as this area is the habitat of several anatomical elements whose lesion can be
functionally and vitally life-threatening. In a patient whose vital functions
are stable, a cervical CT scan can provide a complete lesion assessment,
highlighting any foreign bodies that may have gone unnoticed, and guiding any
surgical exploration.
In this context, we report the case of a man who had a
neck trauma in a road traffic accident, with inclusion of a foreign body which
was revealed at prevertebral level by cervical CT scan. Surgical exploration
was performed to remove the foreign body and explore all the anatomical
structures in the region. The evolution was excellent.
Keywords: Case
Report; Cervical Trauma; Foreign bodies; Surgery
Introduction
Cervical trauma is a potentially serious injury,
characterized by the difficulty of its initial management in the emergency
setting, especially by sharp objects causing open trauma and leaving foreign
bodies behind, with all their lytic, infectious and hemorrhagic complications.
These injuries are always unpredictable and multifocal1.
Mortality has been reported at between 2% and 10%. The
severity and particularity of these lesions call for rapid, precise clinical
analysis, in a context of extreme urgency, using clinical, radiological and
endoscopic methods. These means have undergone considerable technological
progress in recent years2. This has
radically changed management methods, avoiding unnecessary surgical exploration3. In this context, we report the case of a
patient who consulted our department's emergency department for a penetrating
glass wound. The patient underwent a clinical and radiological evaluation prior
to surgical exploration.
Case
report
This is a study of a 50-year-old patient operated on
for a cervical wound, with penetration of a glass-like cervical foreign body in
our ENT and cervico-facial surgery department. The patient was referred by
another hospital.
The patient had no underlying pathology. The trauma
occurred 3 hours prior to consultation in our department.
On general physical examination, the patient was in
good general condition, conscious 15/15 Glasgow score, and hemodynamically and
respiratory stable. On ENT examination,
a paramedian cervical wound measuring approximately 5cm was noted, which had
been sutured at a peripheral hospital to which the patient had first been
referred (Figure 1). The rest of the
ENT examination, and there were no other objective signs of trauma of other
systems. 
Figure 1: Paramedian cervical wound,
which had been sutured
A cervical CT scan with injection of contrast product
was then carried out to assess the lesion and guide the treatment. It revealed
the presence of a prevertebral foreign body, but miraculously all the vascular,
digestive and aerial anatomical structures were intact (Figure 2).
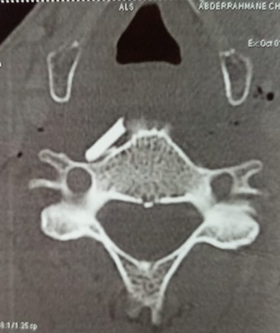
Figure 2: CT scan showing the
presence of a prevertebral foreign body
We started a prophylactic antibiotic treatment with
amoxicillin and clavulanic acid. Given the CT scan data. An indication for
exploratory cervicotomy was made. On preoperative examination, no vascular,
laryngo-tracheal or esophageal lesions were found. In addition, the
sternocleidomastoid muscle was injured. After meticulous dissection using
Halstead forceps, the prevertebral foreign body was found to be a piece of
glass (Figure 3). Next, hemostasis
is ensured and suction drains are placed and closure plan by plan.
Figure 3: Image showing glass-like
cervical prevertebral foreign body
The suction drain was removed the following day. The
evolution was good, no hematoma or other signs of lesions of the cervical
anatomical structures were noted.
Discussion
Neck penetrating wounds are notoriously difficult to
assess owing to the fact that they involve a technically complex region where
several vital structures are located in a limited space. There is still
controversy about the systematic application of specialized diagnostic tests,
including invasive ones, to stable, asymptomatic patients1.
Non-operative management has gained in popularity in
recent years, especially with advances in imaging4.
Cervical region anatomy is distinguished by a number of vital vascular,
neurological, respiratory and digestive structures enclosed by thick, poorly
extensible fasciae. Penetrating trauma may cause a number of arterial lesions,
including arterial transections, AV fistulas, pseudoaneurysms and voluminous
hematomas. But also laryngeal, tracheal and esophageal lesions5.
Alongside the skin, blood vessels are the anatomical
structures most frequently injured, since approximately 25% of penetrating neck
traumas result a vascular lesion. Associated or not with airway obstruction,
cranial nerve damage, and cerebral ischemia due to arterial transection or
occlusion6.
Physical examination is the basis of medical
management. The observation of "strong" clinical signs associated of
hemorrhagic shock requires immediate admission to the operating room. There is
no proven added value to CT imaging prior to hemostasis in the OR. Active
bleeders must be placed in Trendelenburg position to reduce the risk of gas
embolism7.
Missed pharyngoesophageal lesions are among the most
feared pitfalls in cases of penetrating cervical trauma, because the clinical
signs are not always obvious and their treatment is delayed, which can be
life-threatening. Successful conservative management of small esophageal
lesions has been reported by some authors. Signs of a laryngotracheal lesion
include acute respiratory distress, the presence of air bubbles externalized
from the cervical wound, and the occurrence of significant hemoptysis4-9.
The neck is systematized in three compartments (two
lateral and one central). Lateral compartment wounds more often require
surgical exploration. Injuries to the central compartment are responsible for
lesions of the upper aerodigestive tract requiring initial orotracheal
intubation with possible deferred surgical management8.
Advances in CT imaging have led to a radical change in
the management of these types of traumas. With the exception of uncontrollable
hemorrhagic shock, CT scans must be performed systematically on all stable
patients. Its sensitivity is 100%, its positive predictive value 100% and its
negative predictive value 98%. It gives information on the integrity of
vascular, air, digestive and bone structures. Precise arterial and venous
injection times are essential for optimal visibility of the neck's vessels10.
Medical treatments include selective arteriographic
embolization, antibiotic therapy and psychiatric care.
Early administration of antibiotics reduces the rate
of infection. The aim of antibiotic prophylaxis is to prevent gas gangrene due
to anaerobes, particularly Clostridium, also infection due to group A
beta-hemolytic streptococci and infections due to other Gram-positive bacteria.
Antibiotic prophylaxis is usually based on amoxicillin and clavulanic acid (2 g
intravenously, 3 times a day). American guidelines recommend cefazolin, with a
similar spectrum of action11,12.
Psychiatric care is essential for suicide attempts. Tracheotomy
is the reference technique for maintaining a free airway, it has the advantage
of not aggravating a laryngeal lesion13.
Vascular repair is preferable to simple carotid ligation of the internal and
primitive carotid arteries, which has a poorer vital and functional prognosis.
Ligation of the external carotid artery by cervicotomy is indicated if bleeding
cannot be controlled. Similarly, a venous lesion is treated by simple ligation
of the vessel concerned14.
After ensuring that the airway is unobstructed and
hemostasis has been controlled, an assessment of the injury can be made.
Suitable trimming must be the rule in order to avoid the risk of infection, and
skin closure may be deferred. Any foreign body extraction must be carried out
with immediate cutaneous closure on suction drains if the wound is sterile15.
Conclusion
Surgical management of these patients is the
responsibility of specialized multidisciplinary teams. Every open neck trauma
is potentially life-threatening, and requires rapid assessment and detection of
critical injuries, as well as urgent surgical intervention if necessary.
Stable patients are being managed less
interventionistically, based on clinical examination and imaging. When
necessary, it is best to carry out surgical exploration within the first 24
hours, in order to limit the risk of infection and late sequelae.
References
1. Thoma M, Navsaria PH, Edu S, Nicol AJ. Analysis of 203
patients with penetrating neck injuries. World J Surg 2008;32:2716-2723.
2. Steenburg SD, Sliker CW, Shanmuganathan K, Siegel EL.
Imaging evaluation of penetrating neck injuries. Radiographics
2010;30(4):869-886.
3. Schroeder JW, Baskaran V, Aygun N. Imaging of
traumatic arterial injuries in the neck with an emphasis on CTA. Emerg
Radiol 2010;17:109-22.
4. Velmahos GC, Souter I, Degiannis E, Mokoena T, Saadia
R. Selective surgical management in penetrating neck injuries. Can
J Surg 1994;37:487-491.
5. Amirjamshidi A, Abbassioun K, Rahmat H. Traumatic
aneurysms and arteriovenous fistulas of the extracranial vessels in war
injuries. Surg Neurol 2000;53(2):136-145.
6. Nuñez DB, Torres-León M, Múnera F. Vascular injuries
of the neck and thoracic inlet: Helical CT-Angiographic correlation. Radiographics
2004;24(4):1087-1100.
7. Demetriades D, Salim A, Brown C, Martin M, Rhee P.
Neck Injuries. Curr Probl Surg 2007;44(1):13-87.
8. de Régloix SB, Baumont L, Daniel Y, Maurin O, Crambert
A, Pons Y. Comparison of penetrating neck injury management in combat versus
civilian trauma: a review of 55 cases. Mil Med
2016;181(8):935-940.
9. Ngakane H, Muckart D, Luvuno F. Penetrating visceral
injuries of the neck: Results of a conservative management policy. Br
J Surg 1990;77:908-910.
10. Múnera F, Soto JA, Palacio D, Velez SM, Medina E.
Diagnosis of arterial injuries caused by penetrating trauma to the neck:
comparison of helical CT angiography and conventional angiography. Radiology
2000;216:356-362.
11. Mabry RL, Holcomb JB, Baker AM, et al. United States
Army Rangers in Somalia: An analysis of combat casualties on an urban
battlefield. J Trauma 2000;49(3):515-528.
12. Société
francophone de médecine d’urgence. Prise en charge des plaies aux urgences.
Conférence de consensus 2005.
13. Hollier L, Grantcharova EP, Kattash M. Facial gunshot
wounds: A 4- year experience. J Oral Maxillofac Surg 2001;59:277-282.
14. Simmons JD, Ahmed N, Donnellan KA, Schmieg Jr RE,
Porter JM, Mitchell ME. Management of traumatic vascular injuries to the neck:
a 7-year experience at a level I trauma center. Am Surg
2012;78:335-338.
15. Kummoona RK. Missile war injuries of the face. J
Craniofac Surg 2011;22(6):2017-2021.