Management of a Steel Wire Type Cervical Foreign Body Introduced by Penetrating Trauma: Case Report and Literature Review
Abstract
Foreign bodies in the ENT
sphere are a frequent cause of emergency room consults. There are different
introduction mechanisms. Foreign bodies
with penetrating trauma are particularly serious, not only because of the
difficulties often faced in managing them, but also because of the
life-threatening risks of hemorrhage and asphyxia. These risks justify early
management by specialized multidisciplinary team. The accessibility of
complementary examinations and the evolution of their techniques have also led
to a clear improvement in this type of treatment. Their occurrence in a context
of violence may require psychiatric treatment. The prognosis depends mainly on
the length and quality of treatment, but also on the damage caused by the
introduction of these foreign bodies. We report on the management of a patient
with psychiatric history, who consulted the emergency department of our ENT
department, for the introduction of a cervical foreign body in the form of
steel wires. A clinical and paraclinical examination was carried out, enabling
anatomical orientation and evaluation of the patient's general condition. The
patient underwent an exploratory cervicotomy to remove the cervical foreign
body and perform a precise lesion assessment. The patient had a good follow-up
with no post-operative complications.
Key
words: Foreign body; Cervical region; Surgery;
Case Report
Introduction
Foreign bodies are a
frequently encountered pathology in emergency ENT practice. They can be
life-threatening by their type or location. It is a frequent event, especially
in children1. The nature of foreign
bodies varies considerably. It essentially depends on the patient's age, eating
habits and condition2. All types of
foreign bodies can be observed in psychotic subjects, especially those of a
metallic nature. This medical-surgical emergency requires multidisciplinary
management involving clinicians, radiologists and surgeons. With this in mind,
we report the case of a patient with a psychiatric background who arrived at
our department with multiple foreign bodies.
Case presentation
We present the case of a 24-year-old woman, living in an orphanage, who was
admitted in our ENT emergency department for sinking multiple steel wires into
her neck. She had a history of mental disorder, vitiligo, and multiple
hospitalizations for auto mutilation by inserting foreign bodies in the neck
and the vaginal cavity for which she undergone cervicotomy under general
anesthesia one year prior to this episode.
The clinical examination found a conscious patient,
with a stable hemodynamic and respiratory state, without dysphonia or
dysphagia. Upon her inspection, we noticed, additionally to a cervicotomy scar,
metallic foreign bodies sticking out of her neck with infected entry points and
pus release.
A Nasofibroscopy was performed showing no sign of
laryngeal damage. A cervico-thoracic x-ray showed multiple wires above the
thyroid cartilage, one supra-clavicular reaching the right hemithorax, and
another one intra-thoracic (Figure 1).
A cervico-thoracic CT-scan was done objectifying, in addition to multiple
subcutaneous metallic foreign bodies (Figure
2), a metallic wire which has migrated in the supra clavicular area and
reached the carotid region, between the internal carotid artery and the
internal jugular vein and reaching the upper part of the thorax, measuring
approximately 4cm (Figure 3).
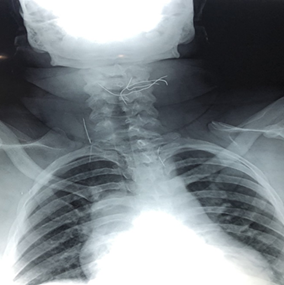
Figure
1: Cervicothoracic
x-ray-frontal view showing multiple cervicothoracic wires (arrow)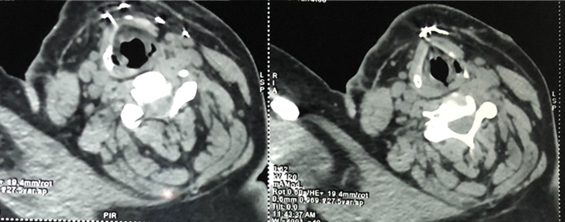
Figure
2: Cervical CT-scan
- cross section showing subcutaneous steel wires in front of the thyroid
cartilage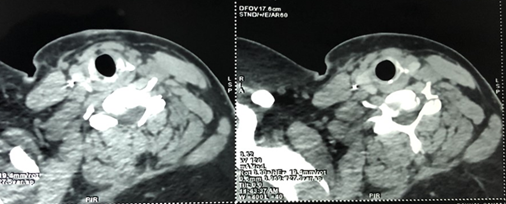
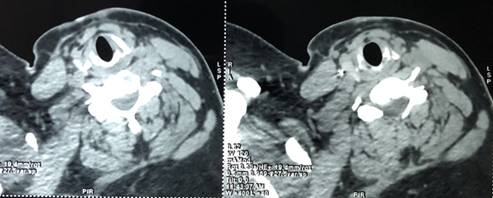
Figure
3: Cervical CT-scan –
cross section showing cervico-thoracic steel wires embedded between the
internal carotid artery and the internal jugular vein
The patient was admitted and hospitalized immediately.
We started an intravenous prophylactic antibiotic treatment based on
Amoxicillin – acid clavulanic with a Tetanus prophylaxis injections and
painkillers before surgical treatment. The
extraction of the foreign bodies was performed under general anesthesia and
lasted 2 hours, by a team composed of ENT surgeons, vascular surgeons and
anesthesiologists.
We started off by extracting the superficial wires
then we proceeded with a Paul-Andre incision. The sternocleidomastoid muscle
was dissected and retracted to expose the vascular axis of the neck. A stiff
granuloma covering the foreign body was highlighted between the internal
carotid artery and the internal jugular vein (Figure 4).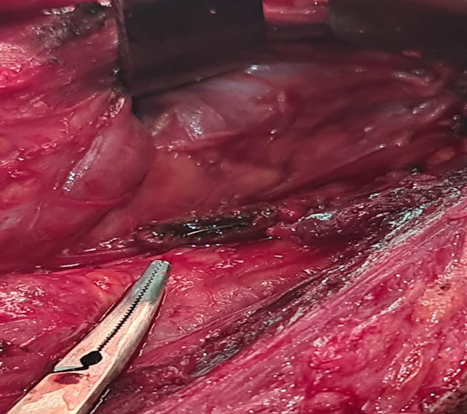
Figure
4: A steel wire
(blue arrow) surrounded by a granuloma (green arrows) between the internal
carotid artery and the internal jugular vein
During the intervention, we noticed that the granuloma
was attached to the internal jugular vein without any cleavage plane. We
proceeded by incising the granuloma in an open book. The wire was extracted (Figure 5) with a Halstead clamp while
the granuloma was not excised given the high risk of vascular injury. A careful
hemostasis was assured. The
postoperative follow up was good with a full recovery within 2 days. The
patient was transferred after to psychiatric department. No complication was
noted after one month follow up.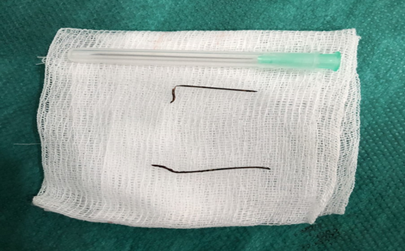
Figure
5: Steel wire
removed from the granuloma, the other one was subcutaneous and easily removed.
Discussion
Generally considered, cervical and upper aero
digestive tract foreign bodies are most common in children under 6 years of
age, with a peak in the 1-4 age group. Boys are the most frequently affected
because of their vivacious3. Among
adults, foreign body injuries often occur in special circumstances: toothless
elderly subjects, patients with psychotic disorders or prisoners who are at
increased risk of ingesting foreign bodies. A century ago, mortality linked to
the ingestion of foreign bodies was 57%. These results can be explained by the
improvement of surgery and endoscopic extraction techniques4.
Apart from underlying psychiatric disorders, diagnosis
is usually straightforward in adults, based on questioning. The situation is
more difficult in children, given that questioning is informative in only 5% of
cases5. Voluntary administration of
foreign bodies is usually seen in prisons, among psychiatric patients or as
part of a suicide attempt. It usually involves multiple foreign bodies
administered at the same time or in close succession6.
The most common ENT functional signs are localized
pain, odynophagia, dysphagia, dyspnea and hyper-sialorrhea. However, these
patients may be asymptomatic7. In all
cases of suspected CE ingestion, a full radiological work-up is essential.
Standard X-rays are the usual diagnostic investigation. Systematically,
patients should be given chest x-rays from the front, neck x-rays from the
front and in profile, with inspiration and the head slightly hyper flexed to
clear the inter-tracheo-vertebral space, and unprepared abdominal x-rays from
the front in the standing position. In addition, CT scans provides greater
precision in determining the exact location of a foreign body8.
The neck includes all the anatomical structures
between the base of the skull and the clavicles. Dealing with penetrating
cervical foreign bodies is based on the systematization of the neck into three
anatomical zones according to the foreign body's entry orifice. Zone I is
delimited by the clavicle and the sternal fork at the bottom, and by the lower
edge of the cricoid at the top. Zone II lies between the lower edge of the
cricoid and the mandibular angle. Zone III extends from the mandibular angle to
the base of the skull9.
For stable patients, zone II offers the advantage of
easier anatomical access and the possibility of surgical exploration via
cervicotomy. Zones I and III encouraged the use of radiological methods of
exploration, given their narrowness and difficult surgical access. The lateral
compartment is the site of vascular lesions, and wounds in this compartment
more often require surgical exploration. Damage to the central compartment is
responsible for lesions of the upper aerodigestive tract requiring initial orotracheal
intubation, with initial monitoring in intensive care and possible delayed
surgical management10.
Specific medical treatments include antibiotic
prophylaxis and psychiatric care. The aim of early prophylactic antibiotics is
to prevent bacterial growth in heavily contaminated tissues. Thus, avoids gas
gangrene caused by anaerobes, especially Clostridium, but also infection caused
by group A beta-hemolytic streptococci and infections caused by other
Gram-positive bacteria, particularly Staphylococcus aureus. Prophylaxis with
amoxicillin and clavulanic acid (2 g direct intravenous, 3 times a day) is
recommended. American guidelines recommend cefazolin, with a similar spectrum
of action. In case of allergy, prophylaxis with clindamycin is indicated (600
mg intravenous infusion, 4 times a day)11,12.
The main risk in these cases is respiratory distress
and hemorrhage. The signs of severity of these cases are therefore dominated by
signs of hypoxemia, which determine the immediate prognosis, leading to
cardiorespiratory failure in the absence of appropriate treatment, and signs of
hemorrhagic shock. The therapeutic surgical approach to be considered generally
if early management is chosen is extraction of foreign bodies, followed by
local care (cleaning, washing), and immediate skin closure with suction drains13.
Conclusion
The management of this type of cervical foreign body
by penetrating trauma is multidisciplinary. It consists after ensuring control
of any eventual hemorrhage and lesion of airways, of performing a radiological
injury assessment to prioritize the damage and guide surgical management.
Psychiatric care is essential in these cases.
References
1. Nikiphorou E,
Demetriou C, Norton S, et al. The
impact of comorbidities and extra-articular manifestations on 10-year mortality
risk in rheumatoid arthritis. results from two multi-centre uk inception
cohorts. Ann Rheum Dis 2015;74:690-691.
2. Sarmiento-Monroy JC,
Amaya-Amaya J, Espinosa-Serna JS, Herrera-Diaz C, Anaya J-M, Rojas-Villarraga
A. Cardiovascular disease in
rheumatoid arthritis: a systematic literature review in latin america. Arthritis
2012.
3. Kacouchia
N, N’gattia KV, Kouassi M, et al. Corps étrangers des voies aéro-digestives
chez l’enfant. Rev Col Odontostomatol
Afr Chir Maxillofac 2006;13(3):35-39.
4. Lefriekh R, Aisse L,
Louzi A, Ridai M, Zerouali NO. Ingestion de corps étrangers. Revue Marocaine de
Médecine et Santé 2003;20(2):52-57.
5. Letard JC. Ingestion de
corps étrangers. Iléus 2003;20:13-15.
6. Letard
JC, Happinono M. Les corps étrangers ingérés et ingestion de toxiques. Acta
Endoscopica 2004;34(5): 671-678.
7. Sahota A, Shandil R, Barmaki A. R, Salama P, Simpson
Nl. Foreign body ingestions: Characteristics and outcomes in a lower
socioeconomic population. Gastrointestinal endoscopy 2006;63(5):154.
8. Kamath P. Bhojwani KM, Prasannaraj T, Abhijith K.
Foreign bodies in the aerodigestive tract-A clinical study of cases in the
coastal belt of South India. Am J Otolaryngology 2006;27:373-377.
9. Monson DO, Saletta JD, Freeark RJ. Carotid
vertebral trauma. J Trauma 1969;9(12):987-999.
10. de Régloix SB, Baumont L, Daniel Y, Maurin O, Crambert
A, Pons Y. Comparison of penetrating neck injury management in combat versus
civilian trauma: A review of 55 cases. Mil Med
2016;181(8):935-940.
11. Merens A, Rapp C, Delaune D, DanisJ, Berger F, Michel
R. Prevention of combat-related infections: Antimicrobial therapy in
battlefield and barrier measuresin French military medical treatment
facilities. Travel Med Infect Dis 2014;12(4):318-329.
12. Dunkel N, Pittet D,
Tovmirzaeva L, et al. Short
duration of antibiotic prophylaxis in open fractures does not enhance risk of
subsequent infection. Bone Joint J 2013;95:831-837.
13. Petersen K, Colyer MH, Hayes DK, Hale RG, Bell RB.
Prevention of infections associated with combat-related eye, maxillofacial, and
neck injuries. J Trauma 2011;71:264-269.