Mandibular Botryoid Cyst with Large Extension, Treated by Decompression and Marsupialization: A Case report
Abstract
The maxillo-mandibular complex is
subject to rare pathologies, such as odontogenic and non- odontogenic cysts and
tumors. The presentation can be clinically symptomatic, with localized edema,
facial asymmetry, paresthesia, dental mobility, gingival discoloration and
pathological fracture of alveolar bone. It can also be asymptomatic,
occasionally discovered during routine radiographic examination. The lateral
periodontal cyst (LPC) is a rare odontogenic cyst that usually appears on the
lateral surface of vital tooth roots and can have a more aggressive
presentation known as botryoid odontogenic cyst (BOC). BOC is a rare
odontogenic pathology, which can be extensive causing bone destruction and
tooth loss. Large cases can be treated surgically, with decompression and marsupialization,
presenting good clinical progress, reduction in symptoms with bone growth
potential, which associated with conventional surgical enucleation, in a
pathology of smaller dimensions, has better prognosis. This study presents a
case of an extensive symptomatic BOC in the mandible, discovered by routine
radiographic examination, and treated by marsupialization and decompression,
and discusses this pathology and the importance of proper management to avoid
tissue and dental damage. The cases must be followed up for years due to the
high possibility of recurrence.
Keywords: Botryoid Cyst; Lateral periodontal cyst; Osseous pathology;
Odontogenic tumor.
Introduction
The lateral periodontal cyst (LPC) is a
rare odontogenic cyst most commonly found in the mandible, between the roots of
the canine and premolar teeth. The botryoid cyst (BOC) is a variant of LPC,
most often affecting middle-aged and older adults, with a multilocular aspect
generated by the spread of concentrations of epithelial remains that results in
an aspect of grape cluster. Although both LPC and BOC can be managed with
simple enucleation, it is worth noting that while first one has an extremely
low recurrence rate, the latter can recur more easily.
Being a cyst of odontogenic origin, the
LPC is considered a rare lesion in the oral cavity, with an occurrence rate of
less than 1% among all odontogenic cysts1.
The diagnosis is based upon radiographic analysis where a drop-shaped
radiolucency with well-defined margins is observed. LPC originates from
epithelial remains and presents a thin keratin layer histologically. Although
it is a rare pathology, it is not a painful lesion. It has a slight female
predilection and is more common in patients between 40 and 70 years of age. It
appears laterally around the roots of vital teeth, more frequently canines and
premolars of the mandible, with its most accepted origin being the remnants of
dental lamina, reduced enamel epithelium and epithelial rests of Malassez. The
preferred treatment plan is enucleation, always emphasizing the importance of
preserving the adjacent dental element2.
The BOC is a variation of the LPC,
gaining its name because it resembles the shape of a bunch of grapes,
morphologically3. Also considered a
rare odontogenic cyst, it is radiographically identified with a multilocular
appearance, due to the presence of epithelial remains in its margin. It has a
higher incidence of occurrence in the mandible, having the same treatment as LPC,
but requiring a more meticulous treatment plan due to its high recurrence rate4.
Although the causative pathogens are
different, it is important that both are treated immediately after diagnosis,
avoiding sequelae such as pathological fractures, infections, local pain and
tooth loss, which could cause major complications to the rehabilitation
treatments5.
Case report
Patient AA, 32 years old male, attended
the maxillofacial surgery clinic referred by a fellow dental surgeon
complaining of an intraoral mass, with a slight change of mucosa color in the
region of mandibular canine and premolars on the right side, associated with
mild pain and mandibular hypoesthesia in the lower right lip and mental region.
The patient, otherwise healthy, was hypertensive, using medication (losartan
and zolpiden), non-smoker and an occasional drinker. He did not report any
local trauma or other previous surgery in the specified region.
Upon clinical examination, an expansive
mandibular lesion was noted, the buccal bone plate presented slight crackling
and no teeth mobility was observed (Figure
1). Radiographic and tomographic examination (Figure 2 & Figure 3)
revealed an ill-defined multilocular radiolucency, with “honeycomb” aspect,
adjacent to the roots of the lower right canine and premolars, without
mandibular base involvement. Pulp vitality test was applied using endofrost
(cold) and gutta percha (heat), revealing vital canine and non-vital premolars.
The differential diagnosis was Ameloblastoma, botryoid cyst and central lesion
of giant cells. 
Figure 1. Intra and extra oral
clinical appearance.
Figure 2. Initial panoramic
radiograph showing multilocular bone appearance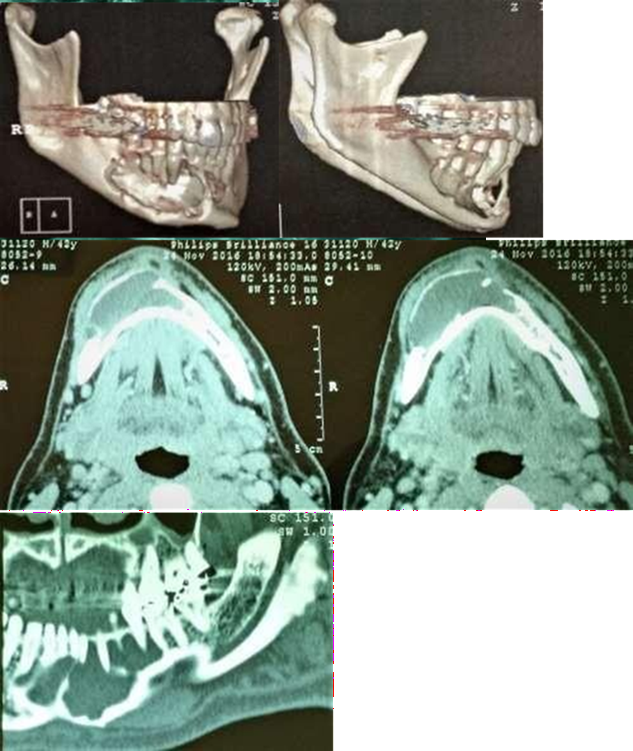
Figure 3. Initial CT scan showing bony lesion
Due to the lesion size and proximity to
neighboring teeth, the patient was oriented to perform endodontic treatment on
the non-vital teeth. Consequently, an incisional biopsy and cyst decompression
were scheduled. The surgical procedure was performed under local anesthesia,
after local antisepsis, aspiration was performed with an 18G needle, returning
a citrus liquid content, then a small vestibular incision was made to access
the cystic cavity. Two fragments were obtained and stored in 10% formalin vial
and sent for histopathological analysis at the oral pathology department at the
Faculty of Dentistry of the University of São Paulo. The surgical incision was
then sutured and a decompression stent was introduced to keep the incision open
for decompression. The patient was instructed to irrigate the cystic cavity 3x
a day with 0.12% chlorhexidine solution (Periogard) to avoid obstruction and
infection. (Figure 4). Shows the
results obtained after 4 weeks of decompression. A notable reduction in
vestibular mass can be visualized in this image and the patient reported a
major pain relief. Future cyst enucleation was decided according to radiologic
evaluation of the cystic size and affected bone.
Figure 4. Cystic decompression result after 4 weeks.
The histological slides (Figure 5) show the presence of multiple
cystic cavities of variable sizes and shapes, and thin walls lined with
non-keratinized stratified squamous epithelium of variable thickness; the
epithelium either consisted of a few cell layers or showed thickening generally
formed by oval, sometimes entangled, plaques. The cystic capsule is
characterized by dense connective tissue that is highly collagenized, with the
deposition of bundles of collagen fibers in various directions. A large number
of blood vessels are noted, sometimes congested and of varying sizes, with
extensive areas of interstitial hemorrhage. In the submucosa, bundles of
striated skeletal muscle and trabeculae of mature bone are noted completing the
analyzed histopathological picture. The result of the histopathological
examination was a botryoid cyst, a variation of the lateral periodontal cyst,
with characteristic stratified squamous epithelium, focal thickening with
mucous cells and a multicystic aspect.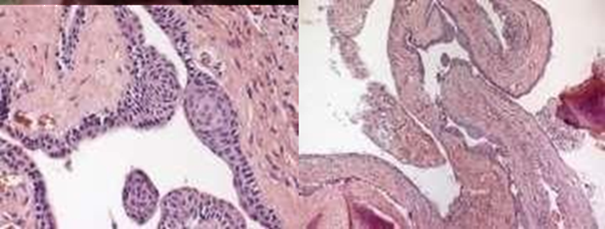
Figure 5. Histologic Slides
Local irrigations and follow-ups were
maintained for 6 months, and a new radiographic examination was performed,
showing notable clinical and radiographic improvement, but still showing
radiolucency adjacent to neighboring teeth (Figure 6). At this time, it was decided to perform a new surgery
for enucleation and definitive treatment as shown in (Figure 7).
Figure 6. Radiographic appearance at 6 months post-op. There is an evident
radiographic sign of bone formation in the peripheral areas.
Figure
7. Enucleation surgery. A vestibular bone defect is
noted in the decompression stent area where irrigation was performed. Cystic
extension decreased, with defined margins. A small releasing incision was made
to permit the complete closure of the defect.
The patient was medicated with
antibiotics (cephalexin), nsaids and analgesics (ketoprofen and paracetamol),
with periodic follow-ups until complete recovery after surgery, which was
uneventful. The patient evolved with complete remission of symptoms and
returned to his normal routine. He is under regular monitoring, remaining
asymptomatic and without radiographic signs of recurrence after 4 years of
control, as shown in Figure 8.
Figure 8. Radiographic examination at 4 years follow-up shows no signs of
recurrence.
Discussion
The BOC is a rare and relatively new
entity, first described by Weathers and Waldron in 19736. It has been defined as a multilocular variant
of LPC, which in turn is defined as a non- keratinized developmental cyst of
the alveolar bone occurring on the lateral aspect of vital teeth7. However, LPC and the BOC are not considered
to be of the same entity by other authors, and the latter is defined as a
multicystic odontogenic lesion with histological characteristics of LPC or cystic
lesion similar to LPC8-9. BOC can
occur at any age, but more usually in individuals above 50 years of age, with a
slight female predilection10-11. The
most frequent location is the mandible, followed by the anterior region of the
maxilla, appearing as a multilocular radiolucency that can grow into
considerable sizes with consequent swelling, pain, paresthesia and other signs11-12. The differential diagnosis for
multilocular radiolucencies include odontogenic keratocyst, multicystic
ameloblastoma, odontogenic myxoma, ameloblastic fibroma, central odontogenic
fibroma and intraosseus mucoepidermoid carcinoma11-13.
An incisional biopsy should be performed to confirm the diagnosis12. BOC shows a high recurrence rate (21.7%),
when compared to LPC (2.4%)14, its
recurrence rate resembles that of glandular odontogenic cysts and odontogenic
keratocysts15-16. The high recurrence
rate can be attributed to the multicystic nature of the cyst, making it
difficult to achieve complete excision, and increases the risk of future
recurrence due to the presence of cystic epithelial remnants after excision17. In a rare presentation, a case with 4
recurrences within 9 years was described in 198918.
Histologically, both LPC and BOC have numerous possible origins, including
cells of rests of dental lamina, epithelial rests of Malassez and reduced
enamel epithelium19. Some authors
suggested that BOC arises from changes in several adjacent cell rests
especially from the post functional cells of dental lamina10, being a polycystic variant of LPC developing
by cystic transformation of multiple islands of dental lamina rests4-19.
Treatment of choice for multicystic bocs
is meticulous surgical excision, with curettage of all cystic epithelium.
Conservative enucleation is not recommended due to the high recurrence rate11. Hence, long-term follow-up is highly
indicated, with radiographic examination20.
It is worthy to emphasize on the importance of pathological categorization and
diagnosis due to different treatment options among different cystic variants.
LPC, for instance, can be treated with simple enucleation with a very low
recurrence rate, BOC requires cystic decompression followed by surgical
excision, whereas ameloblastoma treatment ranges from enucleation to en bloc
marginal resection21.
Conclusion
BOC is a more aggressive variant of
LPC, which presents an extensive lesion clinically and radiographically that,
if left untreated, may lead to tooth loss, pathological fractures and
neurosensory disorders. Initial marsupialization and decompression can be
indicated in cases of large cystic lesions, gradually decreasing the cystic
size and alleviating the clinical symptoms, allowing for future surgical
excision with less morbidity and excellent results.
Ethical disclosures
Protection of human and animal
subjects.
The authors declare that the procedures
followed were in accordance with the regulations of the relevant clinical
research ethics committee and with those of the Code of Ethics of the World
Medical Association (Declaration of Helsinki).
Confidentiality of data
The authors declare that they have followed the protocols of their
work center on the publication of patient data.
Right to privacy and informed consent
The authors have obtained the written
informed consent of the patients or subjects mentioned in the article. The
corresponding author is in possession of this document.
Conflicts of
interest
The authors declare they have no conflicts of interest.
References
1. Karveleas
I, Kalogirou EM, Tosios KI, Nikitakis NG. Synchronous occurrence of two lateral
periodontal cysts in the same patient. Report of a rare case and review of the
literature. J Clin Exp Dent 2020;20(4):418-423.
2. Ramalingam
S, Alrayyes YF, Almutairi KB, Bello IO. Lateral Periodontal Cyst Treated with
Enucleation and Guided Bone Regeneration: A Report of a Case and a Review of
Pertinent Literature. Case Rep Dent 2019;2019:4591019.
3. Gonçalves R, Júnior RO, Borba AM, Ribeiro ANC, Sugaya
NN, Júnior JG. Botryoid odontogenic cyst: case report with etiopathogenic,
diagnostic and therapeutic considerations. Rev Gaúch Odonto 2015;63:337-342.
4. Arora P, Bishen KA, Gupta N, Jamdade A, Kumar GR.
Botryoid odontogenic cyst developing from lateral periodontal cyst: A rare case
and review on pathogenesis. Contemp Clin Dent 2012;3(3):326-329.
5. Meseli SE, Agrali OB, Peker O, Kuru L. Treatment of
lateral periodontal cyst with guided tissue regeneration. Eur J Dent. 2014;8(3):419-423.
6. Weathers
DR, Waldron CA. Unusual multilocular cysts of the jaws (botryoid odontogenic
cysts). Oral Surg Oral Med Oral Pathol. 1973;36(2):235-241.
7. Regezi
J, Sciubba J, eds. Patología Bucal. México: mcgraw-Hill
Interamericana Editores; 2000:301-304.
8. Mendes
RA, Waal IVD. An unusual clinicoradiographic presentation of a lateral
periodontal cyst--report of two cases. Med Oral Patol Oral Cir Bucal.
2006;11(2):185-187.
9. Waal
IVD. Lateral periodontal cystlike lesion--a discussion on the so-called
botryoid odontogenic cyst. J Dent Assoc S Afr. 1992;47(5):231-233.
10. Shear M, Speight PM. Cysts of the oral and
maxillofacial regions. 4th Edition, Blackwell, Munksgaard. 2007.
11. Méndez
P, Junquera L, Gallego L, Baladrón J. Botryoid odontogenic cyst: Clinical and
pathological analysis in relation to recurrence. Med Oral Patol Oral Cir Bucal.
2007;12(8):594-598.
12. Ramer
M, Valauri D. Multicystic lateral periodontal cyst and botryoid odontogenic
cyst. Multifactorial analysis of previously unreported series and review of the
literature. N Y State Dent J. 2005;71(4):47-51.
13. Santos
PPDA, Freitas VS, Freitas RDA, Pinto LP, LBD. Botryoid odontogenic cyst: A
clinicopathologic study of 10 cases. Ann Diagn Pathol. 2011;15(4):221-224.
14. Chrcanovic BR, Gomez RS.
Gingival cyst of the adult, lateral periodontal cyst, and botryoid odontogenic
cyst: An updated systematic review. Oral Dis. 2017;1-8.
15. Chrcanovic
BR, Gomez RS. Glandular odontogenic cyst: An updated analysis of 169 cases
reported in the literature. Oral Dis. 2018;24(5):717-724.
16. Chrcanovic
BR, Gomez RS. Recurrence probability for keratocystic odontogenic tumors: An
analysis of 6427 cases. J Craniomaxillofac Surg. 2017;45(2):244-51.
17. Vidaković
B, Uljanić I, Grgurević J, Perić B, Manojlović S. Botryoid Cyst, a Rare Type of
Odontogenic Cyst. Acta Clin Croat. 2016;55(3):510-514.
18. Heikinheimo K, Happonen, Forssell K, Kuusilehto A,
Virtanen I. A botryoid odontogenic cyst with multiple recurrences. Int J Oral
Maxillofac Surg. 1989;18(1):10-13.
19. Rajendran A, Sivapathasundaram B. Shafer’s Textbook of
Oral pathology. 6th Edition, Elsevier company. 2009.
20. Gurol
M, Burkes EJ, Jacoway J. Botryoid Odontogenic Cyst: Analysis of 33 Cases. J
Periodontol. 1995; 66(12):1069-1073.
21. Brad WN. Oral and maxillofacial Pathology, 2nd
Edition, WB Saunders company. 2002.