Multiple Nodular Condensation from Peripheral Excavations Revealing Septic Thrombophlebitis of Jugular Vein: Think of Lemierre Syndrome
Abstract
Lemierre syndrome is a rare and unknown disease. It is defined as a septic thrombophlebitis of the internal jugular vein or one of its collaterals causing multiple septic pulmonary embolus.
It complicates an otorhinolaryngology infection of bacterial origin allowing the hematogenic invasion by anaerobic bacteria, in most cases fusobacterium necrophorum.
The advent of antibiotics has drastically reduced the incidence and mortality of this disease.
The aim of our work was to recall the pathophysiology, clinical and treatment of this syndrome from a case treated in our department and a review of the literature.
Keywords: lemierre syndrome; necrophorum; hematogenic invasion; pathophysiology; otorhinolaryngology infection
Introduction
Lemierre
syndrome is defined as septic thrombophlebitis of the internal jugular vein
(vji) or one of its collateral causes septic embolus, following an
otorhinolaryngological infection of bacterial or viral origin, allowing the
invasion of blood by an anaerobic bacterium, in most cases fusobacterium
necrophorum1. The advent of
antibiotics has drastically reduced the incidence and mortality of this
disease. Currently, due to its rarity, it is a little-known pathology. The aim
of our work was, from a case treated in our department and a review of the
literature, to recall the pathophysiology, the clinic and the treatment of this
syndrome.
Observation
The
clinical examination finds chest pain and a productive cough. There is a
discreet right jugular venous induration at cervical palpation. The oral cavity
examination shows inflammation of the tonsillar region without phlegmon.
Neurological examination is strictly normal (figures 1,2 and 3).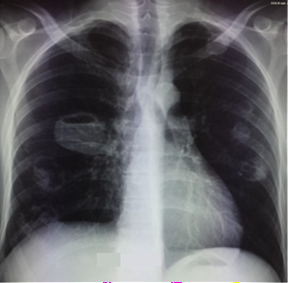
Figure1: chest
radiograph at admission shows multiple bilateral opacities in the exclave.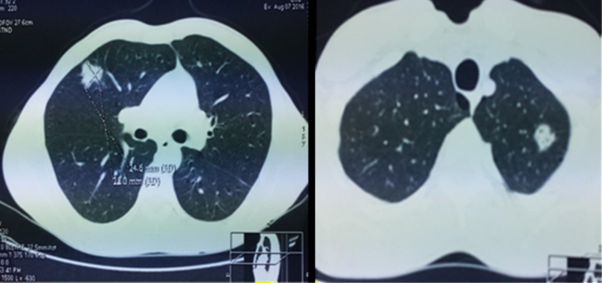
Figure
2: tdm thoracique: multiple bilateral
pulmonary nodules ecaves, emphysemous lung.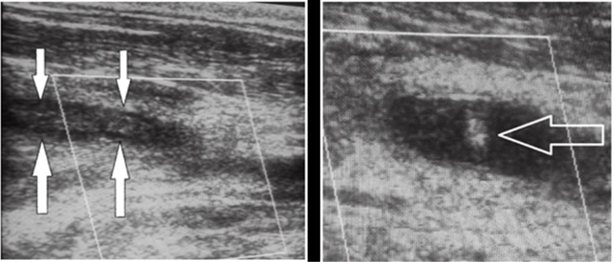
Figure 3: echo-doppler cervical: extensive thrombosis of the right jugular vein and multiple cervical adenopathies.
Biological
balance: infectious and inflammatory syndrome.
Normal
blood gas.
Normal
clotting test.
Hiv serology negative.
In contrast, an anaerobic gram-negative bacillus, identified as fusobacterium necrophorum, grows in one in four blood cultures.
The patient received anticoagulant treatment and a switch to anitivitamine k and probabilistic intravenous bi-antibiotic therapy combining cefotaxim and gentamicine the first two days. Following the results of the additional examinations that point towards a diagnosis of lemierre syndrome, this treatment is modified as follows: ciprofloxacin in ivl + flagyl. The patient’s condition improves with apyrexy after day 5. A doppler ultrasound of the neck vessels shows the persistence of extensive thrombosis of the right jugular vein. The inflammatory syndrome and patient’s condition are significantly improved after 21 days of intravenous bi-antibiotic therapy.
The patient returned home after 21 days of hospitalization, with a per os relay by ciprolon and anticoagulant treatment by vitamin k.
The
radiological evolution was favorable (figure 4) but a widespread
thrombosis of the right jugular vein persisted.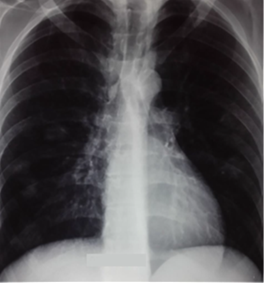
Figure 4: la radiographie thoracique à la sortie
Discussion
Lemierre syndrome is a rare entity, described since
1936 and affecting mainly young healthy adults2.
Its low incidence and the radical change in its prognosis since the advent of
antibiotics have made it a lesser-known pathology. Nevertheless, its acute
character and the risk of serious septic complications invite to make the
diagnosis quickly3.
The clinical picture includes an oropharyngeal, dental, otologic, mastoid or laterocervical infectious starting point. The association with pleuropulmonary manifestations and anaerobic germ sepsis should alert the practitioner. Cervical, ultrasound or ct imaging shows the thrombosis of the internal jugular vein, a key element of the syndrome. Our observation finds a splenomegaly that we can link to this syndrome.
Metastatic infectious sites have also been reported, with a lower frequency, at the cerebromeninged, hepatic, osteo-articular, renal or cardiac level.
On the pulmonary plane, computed tomography finds peripheral nodular condensations of variable size, sometimes excavated, corresponding to disseminated septic embolus. Pleural effusions or pneumothorax are common. The effect on respiratory function may be minimal as in our observation or become much more severe with acute respiratory distress syndrome leading to assisted ventilation.
The detection of the responsible germ can take several days or even weeks due to a 4-day incubation and a difficult culture: fusobacterium necrophorum, commensal gramnegative bacillus from the pharynx, is isolated in hemocultures in about 70% of cases. Other anaerobic germs, fusobacteria or others, are more rarely involved. In any case, antibiotic treatment should be early, active on anaerobic germs and preferably use metronidazole or clindamycin given possible resistance to penicillin.
In our case, even if the antibiogram did not reveal any resistance, it is probably the notion of allergy to penicillin that allowed the installation of such a table. Thus, the early and systematic treatment of any oropharyngeal infectious outbreak by penicillin +/- b lactamase inhibitor explains the epidemiological changes observed.
In addition to antibiotic treatment that will continue for 3-6 weeks, surgical drainage or ligation of the internal jugular vein is rarely required and only affects advanced sepsis. Anticoagulant treatment has not been proven effective, but is usually initiated for a duration of 3 months by many authors. The peripheral nature of the lesions explains the painful component of pulmonary symptoms. An adapted analgesic therapy and respiratory physiotherapy to combat pleural sequelae are part of a comprehensive management of the disease.
Fatal 9 times out of 10 before the age of antibiotics, lemierre syndrome is now a much better prognosis if treatment is early. The hope of complete recovery is therefore very real and confirms the interest of a rapid diagnosis based on the association of oropharyngeal infectious signs with pulmonary symptoms4.
Conclusion
Currently, lemierre syndrome is a rare
and unknown pathology. This is a serious disease that develops in two phases: a
pharyngeal infection followed by a cervical infection causing septic thrombosis
of vji or one of its branches, which itself causes remote septic embolus,
usually pulmonary. Any delay in diagnosis and treatment leads to increased
morbidity and mortality. The most common germ is fusobacterium necrophorum.
The essential paraclinical examinations to be carried out are blood cultures and the cervico-thoracique scan injected. Treatment is primarily medical and based on extended broad-spectrum antibiotic therapy. The role of anticoagulant is not well defined. Surgery is indicated for pharyngeal, cervical or mediastinal abscesses. JIV ligature is currently exceptional5
References
1. Golphe
R, Marin B, Alonso M. Lemierre’s syndrome (necrobacillosis). Postgrad Med J
1999;75(881):141-144.
2. Lemierre
A. On certain septicaemias due to anaerobic organisms. Lancet1936;230:701-703.
3. Sinave
CP, Hardy GJ, Fardy PW: The Lemierre syndrome: suppurative thrombophlebitis of
the internal jugular vein secondary to oropharyngeal infection. Medicine 1989;68(2):85-93.
4. Lacaze
O, Bocquel V, Fournel P, Emonot A. Syndrome de Lemierre: caractéristiques
cliniques et radiologiques d’un diagnostic rare Revue des Maladies
Respiratoires
2000;17(6):1105.
5.
Righini CA, Hitter A, Perrin MA, et al. Syndrome de
Lemierre . Revue de la littérature. Ann Otolaryngol Chir Cervicofac 2014;36(7):1044-1051.