Neurilemoma of the Cervical Plexus: A Rare Case Report and Literature Review
INTRODUCTION
Brachial
plexus schwannoma is a rare cause of chronic cervical mass. It is a benign
tumor developed from Schwann cells in the nerve1.
It is common in the cervical region, especially in the acoustic and vagus
nerve. We present a case of the brachial plexus neurilemoma with a literature
review.
CASE REPORT
We report the case of a
13-year-old female patient with no medical history who presented to our
department with a 5-month history of painless cervical swelling located on the
left side. No signs of cervical compression were reported. The clinical examination
revealed a polylobed firm mass of the left supraclavicular region. It exhibited
greater mobility in superficial layers but showed limited mobility in deeper
layers with no skin changes. The rest of the oto-rhino-laryngoscopy examination
revealed no abnormalities. The ultrasonography showed multiple well-limited
later cervical nodes with regular contours with thickened cortex, the largest
measuring 2.5 cm × 4 cm. The structures repress the internal jugular vein,
which remains permeable. The radiological exploration was complemented by a
computed tomography revealing multiple lymph node-like structures of the left
supraclavicular region measuring 2 cm × 3.8 cm in diameter (Figure 1).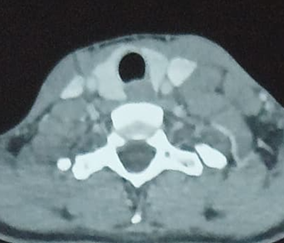
Figure 1: Axial CT scan
The fine needle aspiration cytology (FNAC) of
the mass indicated atypia of undetermined significance. Therefore, the decision
was made to proceed with surgical resection. A lateral cervical incision was
performed posterior to the sternocleidomastoid muscle. The omo-hyoid muscle was
quickly identified after flap dissection. The mass was distant from the
neurovascular bundle and easily dissected from the surrounding structures. A
complete excision was successfully performed (Figures 2 and 3).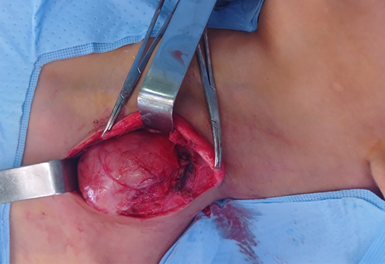
Figure 2: The mass was discovered following a lateral cervical
incision made posterior to the sternocleidomastoid muscle
Figure 3:
Excised mass
before being sent for anatomopathological study.
The histology report indicates
a nodular mass with necrotic rearrangement. The tumor proliferation exhibited
spindle-shaped cells with elongation and an absence of mitosis. The diagnosis
of neurilemoma was favored2,3 (Figure 4).
The post-operative recovery
was uneventful. Following a 1-year follow-up, the patient showed no signs of
recurrence.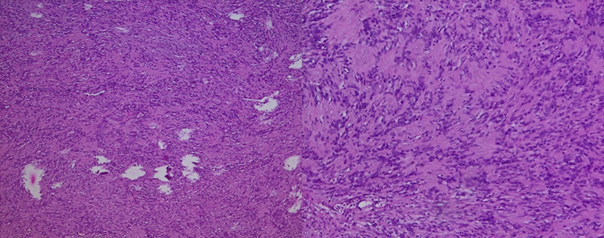
Figure 4: H&E stained sections of the surgically resected
tumor (×20 and ×40 magnification) revealed cytological bland spindle cells with
vague nuclear palisading and a fibrillary background.
DISCUSSION
Schwannomas
of the brachial plexus are considered peripheral nerve sheath tumors4. They usually arise sporadically as benign
tumors, although they are a principal aspect of the two main hereditary tumor
diseases, neurofibromatosis type 2 and schwannomatosis5. Schwannomas are encapsulated, slowly growing
tumors, mobile with commonly no associated neurological deficit, unlike
malignant peripheral nerve sheath tumors, which often produce neurological
deficits6. The brachial plexus could
be studied by ultrasound, evaluating effectively the branches of the brachial
plexus and surrounding soft tissues7.
CT scans can be used to differentiate vasogenic tumors and to exclude
metastatic tumors8. MRI is the
reference type imagery to diagnose brachial plexus problems9, even if it was not demanded in our case
because the patient did not have health insurance.
Fine
needle aspiration and biopsy should be limited if the diagnosis is clinically
suspected due to the risk of neurological damage to the nerve fascicules10. La FNAC usually shows the presence of
spindle-shaped cells and Schwann cells.
Treating
both malignant and benign brachial plexus tumors is essentially surgical, and
schwannomas are no exception11.
Several surgical incisions are proposed depending on tumor size and location.
In our case, we made an anterior supraclavicular incision, which is convenient
for tumors involving the trunk and roots11,12.
The surgical procedure consists of complete resection of the tumor with
conservation of the surrounding nerves, and enucleation is always possible13.
The
postoperative outcome depends on the grade of resection and the pathological
aspect of the tumor; that’s why Tang et al. reported 3 cases of numbness and
paresthesia after the resection of relatively small tumors14.
CONCLUSION
This
case reminds us that schwannomas of the brachial plexus are a differential
diagnosis in supraclavicular tumors. MRI and FNAC could be used in the
diagnostic process, but the confirmation is anatomopathological. Two main
treatment objectives are complete surgical resection and preservation of nerve
function.
REFERENCES
1. Ryu KH, Moon JI, Baek HJ, et al. Brachial plexus schwannoma mimicking
cervical lymphadenopathy: A case report emphasizing imaging features. Medicine 2018;97(42).
2. Nao E, Dassonville O, Bozec A, et al. Cervical sympathetic chain schwannoma. Eur Ann Otorhinolaryng Head Neck Diseases 2012;129(1):51-53.
3. Vučemilo
L, Lajtman Z, Mihalj J, Plašćak J, Lakusic DM, Mužinic D. Brachial plexus
schwannoma- Case Report and literature review. Acta Clinica Croatica 2018;57(2):366-371.
4. Lee, HJ, Kim JH, Rhee SH, GongHS, Baek GH. Is Surgery for brachial
plexus schwannomas safe and effective? Clin Orthop Relat Res 2014;472(6):1893-1898.
5. Pećina-Slaus N, Zeljko M, Pećina HI, et al. Frequency of loss of
heterozygosity of the NF2 gene in schwannomas from Croatian patients. Croat Med
J 2012;53(4):321-327.
6. Ogose A, Hotta T, Morita T, Otsuka H, Hirata Y. Multiple schwannomas in
the peripheral nerves. J Bone Joint Surg Br 1998;80:657-661.
7. Griffith JF. Ultrasound of the Brachial Plexus. Semin Musculoskelet
Radiol 2018;22(3):323-333.
8. Othmane B, Mohamed E, Soufiyane K, Youssef R, Abdelaziz R. Rare schwannomas
of head and neck and review of literature. Indian
J Otolaryng Head Neck Sur 2022;74:6200-6205.
9. Boulanger X, Ledoux J, Brun A, Beigelman C. Imaging of the non-traumatic brachial plexus. Diagnostic and Interventional Imaging 2013;94(10):945-956.
10. Rashid M, Salahuddin O, Yousaf S,
Qazi UA, Yousaf K. Schwannoma of the brachial plexus; report of two cases
involving the C7 root. J Brachial
Plexus and Peripheral Nerve Injury 2013;8:12.
11. Go MH, Kim SH, Cho KH. Brachial plexus tumors in a consecutive series of
twenty-one patients. J Korean
Neurosurgical Society 2012;52(2):138-143.
12. Knight DMA, Birch R, Pringle J.
Benign solitary schwannomas: A review of 234 cases. J Bone Joint Surg Br 2007;89(3):382-387.
13. Horowitz J, Kline DG, Keller SM.
Schwannoma of the brachial plexus mimicking an apical lung tumor. Ann Thorac Surg 1991;52(3):555-556.
14. Tang CYK, Fung B, Fok M, Zhu J.
Schwannoma in the upper limbs. Biomed Res Int 2013;2013:167196.