Non-Traumatic Intra-Thoracic Herniation, Obstruction and Necrosis of Small Bowel Via Right Hemi-Diaphragm Defect: A Clinical Image
Traumatic rupture of diaphragm occurs in 5% of trauma cases which can lead to herniation of abdominal contents into thorax however there are not many reported cases of non-traumatic herniation of abdominal contents into thorax in literature. I present a CT thorax image of a 68 years old man, who had non-traumatic herniation and necrosis of small bowel into thorax. He had a known long standing 9 cm right hemi-diaphragm defect. His main presenting complaints were sudden onset severe abdominal pain when he woke up at his home with no history of trauma. The patient underwent emergency laparotomy followed by small bowel resection and hemi-diaphragm hernia repair. He made a remarkable recovery post-operatively and his bowel function improved and was discharged with follow up plans with the surgeons.
As we can see in the CT slice (pre-operative), there is fluid filled loop of small bowel which appears to have been obstructed (red arrow) in close vicinity of the heart. This loop of small bowel demonstrates poor mural enhancement and surrounding free fluid which is suggestive of bowel ischaemia but there is no evidence of free gas to suggest perforation.
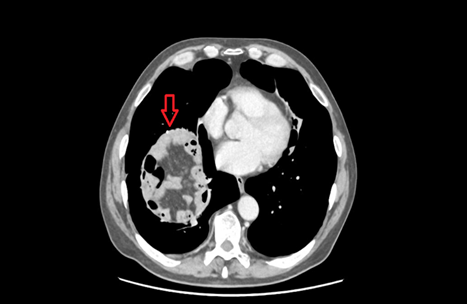
Figure 1. Transverse plane of CT Chest
revealing fluid filled obstructed loop of small bowel marked by red arrow with
evidence of bowel ischemia.