Paraneoplastic Nephrotic Syndrome in a Teenager with Ovarian Teratoma: Successful Treatment with Tumor Resection and Ovarian Tissue Preservation
ABSTRACT
Nephrotic syndrome
is typically associated with primary glomerular diseases but can occasionally
manifest as a paraneoplastic phenomenon. We present the case of a 14-year-old
girl who developed nephrotic syndrome accompanied by significantly elevated CA 19-9
levels. She was subsequently found to have a 7 cm mature ovarian teratoma.
Despite a non-diagnostic renal biopsy, imaging studies and tumor marker
analyses guided the decision to surgically remove the tumor while preserving
ovarian tissue. Postoperatively, her nephrotic syndrome resolved completely,
and CA 19-9 levels normalized within a month. This case underscores the
importance of considering paraneoplastic causes in unexplained nephrotic
syndrome and highlights the critical role of timely diagnosis and a
multidisciplinary approach in achieving full recovery.
Keywords: Paraneoplastic
nephrotic syndrome; Ovarian teratoma; Pediatric nephrotic syndrome; Renal
biopsy; Tumor resection; Remission
INTRODUCTION
Paraneoplastic
phenomena represent an intriguing interplay between tumors and systemic
manifestations, often complicating diagnostic and therapeutic pathways. In
nephrotic syndrome, these associations can manifest as immune-mediated injuries
to the glomeruli, triggered by secreted tumor products or immune responses.
Understanding these rare connections is essential for timely intervention and
improved outcomes1.
Nephrotic syndrome, commonly linked to primary glomerular diseases, can occasionally arise as a paraneoplastic phenomenon, particularly in the presence of systemic conditions such as neoplasms1,2. While rare in pediatric patients, identifying paraneoplastic nephrotic syndrome is vital, especially when tumor markers are elevated without an apparent cause3.
This report
describes a 14-year-old girl diagnosed with nephrotic syndrome associated with
a mature ovarian teratoma. The case highlights the diagnostic challenges and
clinical importance of recognizing paraneoplastic nephrotic syndrome,
particularly in cases with unexplained etiology and elevated tumor markers. It
also underscores the value of a multidisciplinary approach that integrates
clinical, imaging, and pathological evaluations for early diagnosis and
effective management.
CASE
REPORT
A 14-year-old female
presented with periorbital and lower limb edema. Laboratory evaluations
revealed significant proteinuria, hypoalbuminemia, and hyperlipidemia, leading
to a diagnosis of nephrotic syndrome. Renal biopsy was inconclusive1. Further evaluation, including abdominal
ultrasound and MRI, revealed a 7 cm mass in the right ovary with benign imaging
features (Figure 1). Elevated serum CA 19-9 levels were detected, while
other tumor markers remained within normal limits.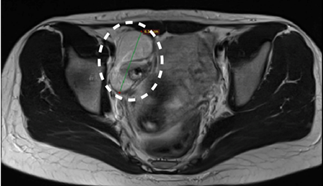
Figure 1: Axial Magnetic
Resonance Imaging (MRI) reveals a well-defined ovarian mass in the right
adnexa, which is consistent with a mature ovarian teratoma. The lesion exhibits
benign imaging characteristics without evidence of invasion
The patient
underwent surgery to excise the right ovarian tumor via a Pfannenstiel
incision, preserving the adjacent normal ovarian parenchyma. Peritoneal fluid
samples obtained pre- and post-excision, as well as after peritoneal lavage,
showed no evidence of neoplastic cells (Figure 2).
Figure
2: Intraoperative image of the resected mature ovarian
teratoma, demonstrating its encapsulated and well-circumscribed appearance. The
tumor was surgically removed with preservation of adjacent ovarian tissue Postoperatively,
the patient achieved complete remission of nephrotic syndrome, which has
remained stable for one year. Histopathological examination confirmed the
diagnosis of a mature ovarian teratoma. Serum CA 19-9 levels normalized within
one month of tumor resection3.
The
histopathological findings provided essential confirmation of the diagnosis,
supporting the benign nature of the mature ovarian teratoma. No evidence of
malignancy or metastatic cells was observed in the intraoperative cytological
evaluations of peritoneal fluid samples. These results validated the hypothesis
of a paraneoplastic mechanism and reinforced the decision to preserve adjacent
ovarian tissue, which is critical for maintaining long-term reproductive health
in young patients. Furthermore, the benign nature of the tumor underscores its
systemic effects as being immune-mediated rather than directly invasive.
DISCUSSION
This case
demonstrates the rare association of nephrotic syndrome with an ovarian
teratoma as a paraneoplastic phenomenon. Such occurrences are rare in pediatric
patients and require a high index of suspicion for timely diagnosis and
treatment4,5.Paraneoplastic
nephrotic syndrome is often attributed to tumor-secreted products, including
cytokines, growth factors, or antigens, which induce immune-mediated glomerular
injury. In this patient, the elevated CA 19-9 levels and the presence of an
ovarian teratoma suggest that the tumor triggered an immune response, resulting
in glomerular damage3. While
mature teratomas are generally benign, their potential to elicit systemic
effects underscores the complexity of their biological activity4.
Diagnosing
paraneoplastic nephrotic syndrome is challenging due to its rarity and the
absence of specific markers linking the tumor to nephrotic syndrome. The
utility of renal biopsy in such cases is debated, as histological findings
often fail to distinguish primary nephrotic syndrome from paraneoplastic
variants1,2. In this
case, the non-diagnostic renal biopsy, along with the identification of a
benign ovarian tumor and elevated tumor markers, was critical in diagnosing the
paraneoplastic condition.
This case
highlights the importance of thorough evaluation in nephrotic syndrome of
unexplained origin, particularly in the presence of elevated tumor markers.
Imaging studies and tumor marker analysis should be integral to the diagnostic
process. Early recognition and surgical excision of the underlying tumor can
lead to complete remission of nephrotic syndrome, as demonstrated here2. Preservation of ovarian tissue during surgery
was crucial for the patient’s long-term reproductive health, especially given
her young age4,5.
Although
paraneoplastic nephrotic syndrome has been reported in association with various
malignancies, including Hodgkin’s lymphoma and renal cell carcinoma, its
occurrence with benign ovarian teratomas is exceptionally rare4,5. The limited cases
described in the literature underscore the potential for benign tumors to cause
significant systemic effects through paraneoplastic pathways. Further research
and clinical studies are necessary to better understand its pathogenesis and
establish reliable diagnostic markers5.
CONCLUSION
This case underscores the importance of
evaluating potential neoplasms in nephrotic syndrome of unexplained origin,
particularly in the presence of elevated tumor markers. The complete resolution
of nephrotic syndrome following excision of a mature ovarian teratoma confirms
the tumor’s role in this paraneoplastic phenomenon, serving as a diagnostic
criterion. The role of renal biopsy remains a subject of debate, requiring
individualized consideration based on clinical findings. Early diagnosis and
multidisciplinary management are critical for optimal outcomes, as demonstrated
in this case, where timely identification and surgical treatment led to full
recovery2,4,5. This case reinforces
the need to consider paraneoplastic causes in complex nephrotic syndrome
presentations, given their potential for significant systemic impact and
reversibility with appropriate treatment.
REFERENCES
1.
D’Agati VD, Kaskel FJ. Nephrotic syndrome in
children. The. Lancet 2012;379:2176-2188.
2.
Schiller M, Larrieu S. Paraneoplastic nephrotic syndrome: An overview.
Pediatric Nephrology 2021;36:511-518.
3.
Brennan MP, Kaplan MM. Nephrotic syndrome and its association with
malignancy. Pediatrics and Nephrology 2013;28:631-639.
4. Cimino JJ, de Montalvo E. Ovarian teratomas and their associated systemic
effects: Case report and review of the literature. International Journal of
Pediatric Endocrinology 2007;200717.
5.
Kilic AT, Unal O. The role of ovarian teratomas in the pathogenesis of
paraneoplastic nephrotic syndrome. Pediatric Nephrology 2016;31:1201-1203.
6.
Golubovic D, Vukovic A. Paraneoplastic nephrotic syndrome: An
under-recognized entity. Nephrology Dialysis Transplantation 2020;35:604-609.