Primary Intra-Orbital Hydatid Cyst as A Cause of Unilateral Exophthalmos: A Case Report
Abstract
Introduction: intra-orbital hydatid cyst is a very rare pathological entity that affects children and the young adults. Hydatid cysts rarely appear isolated in the orbital cavity without involvement of other organs. Most of these are situated in the supéro-lateral and supéro-medial angles of the orbit. Inferiorly located cysts are very uncommon.
Case report: we report a case of 5 years male patient who presented with left eye exophthalmos, and was subsequently diagnosed with left intra-orbital hydatid cyst, treated surgically using a combined endoscopic and external approach.
Discussion: intra-orbital hydatid cysts are a very rare occurrence. Clinical presentation of intra-orbital hydatid cyst is dominated by proptosis and a decrease in visual acuity. Complete surgical excision is difficult, and evolution is generally better when the treatment is early before the installation of irreversible optic atrophy.
Conclusion: although very uncommon, the
intra-orbital hydatid cyst must be evoked in endemic countries. Clinical and
imaging characteristics should be used to further confirm the suspected
diagnosis.
Keywords: orbital cyst; hydatid cyst; intra-orbital hydatid cyst; hydatidosis
Introduction
Orbital hydatid cysts are a rare
localization of the echinococcus granulosus parasite, whose hosts are sheep and
dogs. Morocco is an endemic country where hydatidosis is still rife1,2. In 1 to 2% of cases, the parasite is
localized in the orbit1,3. The main
clinical sign of orbital cysts is exophthalmos. The contribution of imaging,
ultrasound and especially ct imaging, is essential for pre-operative diagnosis.
Furthermore, serology is insufficient and treatment is essentially based on
surgery
Case report
We report the case of a 5 years old male
patient without a medical history, who presented to our department for the
appearance of isolated exophthalmos of the left eye over a three-month period,
with no other associated signs, in particular no decrease of visual acuity, and
no sino-nasal symptoms (figure 1).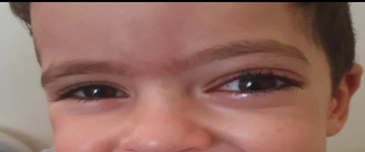
Figure 1. Preoperative image of the patient
showing left exophthalmos
Clinical examination found a prominent
left eye exophthalmos. Nasal endoscopy discovered no abnormalities, and the
ophthalmological examination showed stage 2 papillary oedema in the left eye.
The craniofacial ct-scan (figure 2)
showed grade 3 exophthalmos with a thickening and infiltration of the left
palpebral soft tissues, with evidence of a medial extra conical collection of
mild density, measuring 31 x 22 mm and extending over 21 mm, with a mass effect
on the superior rectus muscle, which was tumefied and compressed. It also had a
mass effect on the ipsilateral optic nerve, which was discreetly swollen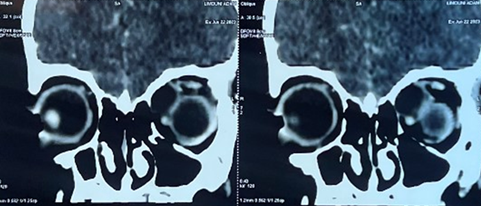
Figure 2. Coronal ct scan images showing the
hypodense mass and its effect on the globe
The orbital mri showed an oval,
well-limited left intra-orbital process, with regular contours and
extra-conical development, in hypo-signal in t1-weighted images, and in
homogenous hyper-signal in t2 weighted images, not enhanced after gadolinium
injection, and measuring 31 x 17 mm extended over 17mm, evoking a neuro-fibroma
or a schwannoma (figure 3).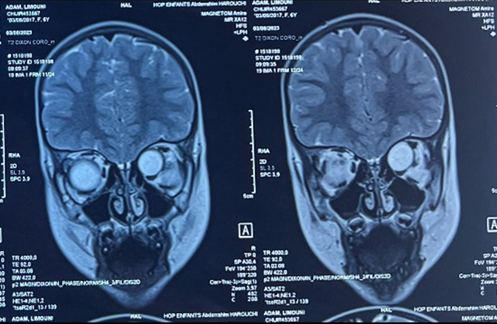
Figure 3. T2-weighted coronal images of the orbital mri scan showing the hyperintense mass located in the superior and medial part of the left orbit
The case file was discussed with the
ophthalmologists, and the decision was to preform surgical excision of the
mass. The surgery was performed by a senior ent surgeon, and a combined
approach was used, involving both endoscopic surgery and an external approach.
Through endoscopic exploration of the left nasal fossa, the lamina papyracea
was opened, thus discovering the mass, which was then dissected anteriorly and
medially.
An external approach was then used, by
way of an eyebrow incision. The mass was discovered in the orbit, and was
adherent to the superior oblique muscle and the optic nerve posteriorly. During
the intervention, the mass was ruptured, revealing that it was in fact a
hydatid cyst, with the exteriorization of the outer pericyst. Because of its
adherence to the optic nerve and to the superior oblique muscle, the excision
of the cyst in totality was deemed too risky. We decided to hollow out the cyst
as much as possible. Pathological examination of the excision tissues confirmed
the diagnosis of a hydatid cyst of the orbit.
Immediate post-operative follow-up found
a paresis of the superior oblique muscle, without diminution of the visual
acuity. The patient underwent adapted physiotherapy, and had recuperated
completely after a month. An abdominal ultrasound was performed, but didn’t
find any sign of hydatid cysts in the liver. Albendazole was prescribed after
the surgery for a period of 3 weeks, to diminish the risk of a relapse.
The follow-up examination, at one month
after surgery, found a significant reduction of the exophthalmos, with a
correct function of the superior oblique muscle. The aesthetic outcome was also
very good (figure 4). Subsequent follow-ups over a six-month period
found no clinical sign of a local recurrence.

Figure 4. Image of the patient
post-operatively (left) and after one month of surgery (right) showing a
remarkable regression after treatment
Discussion
Hydatid cysts
are most commonly located in the liver (60%-70%) and the lungs (20%)4,5. The incidence of intra-orbital hydatid
disease is extremely low, and accounts for 1 to 2% of all hydatid cysts4-8.
The symptoms
include progressive exophthalmos with or without pain, disturbance in ocular
motility, visual deterioration, and chemosis6,7,9.
Orbital involvement is usually unilateral, without right or left dominancy4,5. Typically, an orbital hydatid cyst is
unilateral and can occur with or without other localizations of hydatid cysts7,9. It is usually localized in the superior
part of the orbit, either medially or laterally, and more often than not
affects the motility of the ocular globe1,8,10-13.
On ct, the
orbital hydatid cyst is typically seen as a unilocular, well-defined,
non-enhancing homogeneous cyst with low density, similar to the aspect of the
vitreous body1,14-16. Mri examination
is especially useful to rule out other possible cysts of the orbit. The hydatid
cyst appears as a well-contoured lesion which had a low signal on t1-weighted
images, and a high signal on t2-weighted signals1,14.
In both ct and mr imaging, peripheral rim enhancement is seen after the
injection of a contrast product6,17.
Surgery is the
primary treatment in these cases5,10.
Complete excision is the treatment of choice, but in case of intra-operative
rupture of the cyst, abundant irrigation with saline solution and hydrogen
peroxide should be used to minimize the risk of a recurrence18,19. Anthelmintic treatment is an essential
component of the management of these cases, and should ideally be started 2 to
4 weeks before surgery, or as an adjuvant to surgery, to diminish the risk of
recurrence1,8,18.
Conclusion
Although it is
exceptional, this unusual location of hydatidosis is an important entity, due
to its repercussions, mainly functional. Thus, it should always be thought of
in endemic countries. Preventive measures on the modes of contamination and
general hygiene measures are primordial in these cases, and are the basis for
the eradication of this disease.
References
19. Aloua
r, slimani f. Calcified hydatid cyst of the orbit. J pediatr surg case rep
2021;64:101708