Primary Intraorbital Hydatid Cyst: Case Reports
ABSTRACT
Background : Hydatid cyst is a chronic helminthic parasitic
disease.It is endemic in Morocco.The orbital involvement of isolated hydatid
cysts is a very rare pathological entity, affecting children and young adults
living in rural areas.
Materials and Methods: These are 3 cases report of primary
intraorbital hydatid cysts , collected over a 6-year period from 2019-2024 in
the maxillofacial surgery department at CHU Ibn Rochd in Casablanca.
Discussion: Intra orbital hydatid cysts are very uncommun. Symptoms
include progressive exophthalmos with or without pain, disturbance of monocular
motility, deterioration of vision up to and including blindness, and
inflammatory chemosis.Surgery is imperative, although complementary medical
treatment is useful in most cases to prevent relapse.
Keywords: Hydatidosis; Hydatid cyst; Intra orbital cyst; Unilateral
exophtalmos
INTRODUCTION
Hydatid cyst is a
chronic parasitic disease caused by the cyst-forming tapeworm Echinococcus
granulosis. It is endemic in several parts of the world, including our country (Morocco),
the Middle East, India , South America, Turkey and southern Europe. Humans are
accidental hosts through ingestion of viable eggs. The intra-orbital hydatid
cyst is a very rare pathological entity, affecting youngsters living in rural
areas. In most cases, the diagnosis is made by imaging (ultrasound, CT and MRI).
Treatment is based essentially on surgery, usually combined with medical
therapy. Our case series inclunding 3 cases of primary intraorbital hydatid
cysts collected over a 6-year period in our department is the largest of its
kind, with a wide range of clinical presentations.
CASE REPORTS
All our patients are female and reside in a
rural area.
All our patients
underwent paraclinical examinations in search of another location and no
abnormalities were found.
Case Report 1
A 13-year-old
adolescent presented with progressive, chronic (4 years) and non-pulsatile
unilateral proptosis of the right eye. On clinical examination, a 20 mm
non-axial right exophthalmos was noted; palpation revealed a deep,
non-pulsatile, slightly tender, firm superior-internal orbital mass with
decreased visual acuity without chemosis or oculomotor disturbance.Computed
tomography revealed a 26 x 42 mm isodense retrobulbar cystic mass at the level
of the superior-internal angle of the right orbit, with a thick calcified wall
pushing the optic nerve backwards.
Hydatidosis serology
was positive.
The patient underwent
exeresis of the cyst by internal paracanthal obitotomy, followed by treatment
with albendazole 200 mg daily for 6 weeks. Complete irrigation of the orbit
with H2O2 hydrogen peroxide was performed following cyst rupture. Clinical evolution was favorable (disappearance of
exophthalmos and return of vision).
Case Report 2
67-year-old woman
with asthma and type II diabetes presented with chronic ocular pain and
headaches (8 months) followed by the appearance of chemosis, exophthalmos and
rapidly progressive visual deterioration. Clinical examination revealed an
irreducible, non-tender, non-thrilling superolateral mass responsible for axial
exophthalmos, chemosis, cleft eyelid, corneal dystrophy, ophthalmoplegia,
abolished photo-motor reflex and blindness (Figure
1).
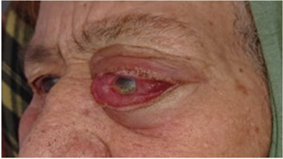
Figure 1. Photos of an elderly woman with an orbital
hydatid cyst revealed by chronic exophthalmos, inflammatory chemosis and
blindness.
Imaging (CT and MRI)
revealed a 35 x 28 x 27 mm left extraconical cystic formation pushing back a
deformed globe, the muscular cone and the lacrimal gland with grade III
exophthalmos and optic nerve stretch (Figures
2 and 3).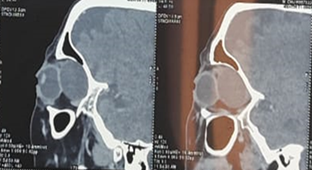

Figure 2. Orbital CT scan showing a well-limited
extra conical formation with regular contours and non-enhanced liquid density
after injection of contrast medium measuring 30 x 26 mm extended over the eye.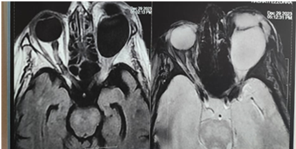
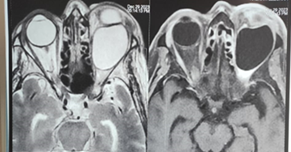
Figure 3. Orbital MRI : Extra conical
intraorbital cystic formation with thin and regular wall in hyposignal on all
sequences not enhanced after gadolinium injection measuring 35x28x27 mm, the
content is in T1 hyposignal, T2 hypersignal disappearing on the FLAIR sequence
without restriction of dissidence or enhancement after injection of gadolinium
this mass exerts a mass effect on the intraorbital structures (the eyeball, the
superior rectus muscle and the optic nerve).
Hydatidosis serology
was positive. Enucleation of the cyst via the superolateral approach with
abundant lavage with hypertonic saline solution following cyst rupture (Figure 4).

Figure 4. Immediate post-operative photos after
enucleation by left lateral orbitotomy
As a preventive
measure, the patient received albendazole for 6 months.The clinical evolution
was marked by the disappearance of exophthalmos and chemosis (Figure 5). 

Figure 5. Ilage of the patient after two months of
surgery showing a remarquable regression of exophtalmos et chemosis after the
treatment
Case Report 3
43-year-old woman
with no particular pathological or trauma history, presenting with rapidly
progressive left exophthalmos evolving for one month. Clinical examination
revealed painless, irreducible, non-pulsatile, non-axial exophthalmos without
thrill, with limited globe elevation, decreased visual acuity, exotropia and
papilledema.
Imaging (CT and MRI)
revealed a cystic lesion of the superior-internal angle of the left orbit,
measuring 29x 20 x 17 mm, at the thin-walled level of the medial rectus muscle,
pushing the eyeball and nerve outwards and causing grade I exophthalmos.
Hydatid serology was
negative.Enucleation of the cyst was carried out via the internal paracanthal
route, without breaking the cyst wall (Figure
6).
Figure 6. Photo of
cyst delivery via internal paracanthal approach
Post-operative
follow-up was favourable (disappearance of exophthalmos, good ocular motility
and return of good visual acuity).
DISCUSSION
It is well known that
hydatid cysts affect the liver and lungs in 50-70% and 20-30% of cases
respectively; however, they can appear in any part of the human body1,2. The
orbit represents a rare (1%) but not exceptional location for these cysts in
endemic countries such as Morocco3,4. Commonly, orbital hydatid cysts are primary
and unilateral, manifesting clinically as exophthalmos of insidious,
non-pulsatile onset, with no palpable thrill; often non-axial and painless5.
It is frequently
diagnosed early in children, due to the limited space in the orbit6. In
addition to exophthalmos, the mass effect resulting from cyst enlargement leads
to periorbital pain, chemosis, restriction of extraocular motility, compressive
optic neuropathy and optic atrophy, which may lead to reduced visual acuity or
even blindness7.
Until today, no case
of bilateral orbital hydatid cyst has been reported. The cyst is most often
located in the left orbit.
Orbital hydatid cysts
tend to involve retrobulbar tissues, either inside the muscular cone or outside
in the upper angles of the orbit. Inferior location remains exceptional.
Diagnosis is made in most cases by imaging
(ultrasound, CT and MRI), but MRI represents the best paraclinical examination
as it can rule out other lesions8-10.
Infact : A CT scan reveals a round or oval lesion, hypodense,
homogeneous, with regular boundaries and denser contours (capable of taking
moderate contrast).MRI provides a better analysis of the cyst, which appears
hypointense in T1 and hyperintense in T2, and the wall is enhanced after
injection of gadolinium.
The serological tests
used in difficult cases - enzyme-linked immunosorbent assay (ELISA) or Western
Blot - can only affirm the diagnosis.Consequently, a negative test does not
rule out the diagnosis.
Confirmation relies
on histological study and/or direct identification of Echinococcosis granulosus
protoscolae or hooks in cyst aspirates, but it should be noted that the clear
appearance of cystic contents found intraoperatively is highly suggestive. However,
in the absence of an epidemiological context, negative serology or inconclusive
imaging, other differential diagnoses must be eliminated.
Several differential
diagnoses may be evoked, including: a reworked cavernous angioma, a mucocele, a
dermoid cyst, a colobomatous cyst, an epidermoid cyst and a post-traumatic
hematoma.
In the absence of
enucleation, the hydatid cyst will progressively form a thick, adherent shell
with no cleavage plane with surrounding tissues, making complete dissection
difficult.
Extracranial or
transcranial approaches can be used to excise orbital hydatid cysts.
Depending on the
location of the cyst, there are several approaches, including rhinotomy
(ideally in the case of an inferointernal cyst), orbitotomy (lateral or
paracanthal, or medial anterior supra superciliary).
Because of its complexity and thin wall, the
orbital hydatid cyst often ruptures, causing severe anaphylaxis.It is therefore
advisable to administer albendazole 2 weeks to 1 month before surgery, as an
adjunctive treatment to reduce the risk of relapse1.
Scholastic agents (e.g. 15% hypertonic saline, 0.5% silver nitrate, 30%
hydrogen peroxide, 95% ethanol) can be instilled into the cyst immediately
prior to surgery, or at the time of dissection of the mass and orbital fat
above the cyst head, using absorbent cotton soaked in one of these solutions,
or at the time of cyst rupture to prevent further spread or anaphylactic
reaction (although direct mortality from echinococcosis is almost nil).
Indeed, the scolices
present in the surgical field will be destroyed by osmotic desiccation.
Not forgetting the anaesthetist, who will need
to be rapidly informed in order to take precautionary measures such as antihistamines
and/or corticoids.
Finally, orbital
hydatid cysts have a good prognosis if treated early12.
The evolution is
generally marked by the progressive disappearance of functional signs.
Recommandation
1. Orbital
hydatid cysts should be considered as a differential disease in anyone
presenting with unilateral proptosis and living in livestock-raising areas13.
2. Adjunctive treatment by albendazole is
preconised because complete excision of the lesion is difficult, and may lead
to cyst rupture and subsequent complications.
3. The best outcome is achieved when the
disease is treated early, before irreversible optic atrophy sets
in.
REFERENCES
1. Kumar
M, Viraat H, Prakash A, Chandra SB, Anil K. Neglected case of primary
intraorbital hydatid cyst. Neurology
India 2022 ;70(1):337-339.
2. Debela
AS, Abore KW, Worke AB, Wendimagegn ST. Primary intra-orbital hydatid cyst: A case
report of a rare cause of exophthalmos. Int Med Case Rep J 2024;17:89‑92.
3. Aloua
R, Slimani F. Calcified hydatid cyst of the orbit. J Pediatric Sur Case Rep 2021;64:101708.
4. Motlagh
MF, Aghdam HJ, Motlagh BF. Primary orbital hydatid cyst: A case report. Acta
Medi Iran 2017;55(8):530‑532.
5. Chtira
K, Benantar L, Aitlhaj H, Abdourafiq H, Elallouchi Y, Aniba K. The surgery of
intra-orbital hydatid cyst: A case report and literature review. Pan African
Medical Journal 2019;33:167.
6. Abdoulaziz
S, Kouda F, Iken M, et al. Le Kyste Hydatique Orbitaire Primaire : Une Cause
Rare D´exophtalmie. PAMJ Clinical Medicine 2020;3:16.
7. Chtira
K, Benantar L, Aitlhaj H, Abdourafiq H, Ellalouchi Y, Aniba K. The surgery of
intra-orbital hydatid cyst. Pan Afr Med J 2019;33:167.
8. Abdoulaziz
S, Kouda F, Iken M, et al. Le kyste hydatique orbitaire primaire. PAMJ Clinical
Med 2020;3:16.
9. Oztekin
PS, Yilmaz BK, Gokharman FD, Kosar PN. Primary orbital hydatid cyst: Computed
tomography and magnetic resonance imaging findings. Singapore Medical J
2014;55(11):184‑186.
10. Kahveci
R, Sanli AM, Gurer B, Sekerci Z. Orbital hydatid cyst: Case report. JNS 2012;9(1):42‑44.
11. Al-Muala
HD, Sami SM, Shukri MAR, Hasson HK, Alaboudy AT. Orbital Hydatid Cyst. Annals
of Maxillofacial Surgery 2012;2(2):197.
12. Eckert
J, Deplazes P. Biological,
Epidemiological, and Clinical Aspects of Echinococcosis, a Zoonosis of Increasing
Concern. Clinical Microbiology Reviews 2004;17(1):107‑35.
13. Krifa
MI, Souai Z, Jdidi R, Saadaoui K, Krifa H. Le kyste hydatique de l’orbite : à
propos de deux cas. Neurochirurgie 2019;65(2‑3):121‑22.