Rare Presentation of Pleural Mesothelioma with Associated Dysphagia in an Elderly Female Cement Trader and the Resultant Diagnostic Challenges: A Case Report
Abstract
Mesotheliomas are rare mesenchymal tumours that
arise from the neoplastic proliferation of mesothelial cells lining various
body cavities. Dysphagia is a rare complication of advanced mesothelioma
usually occurring as a result of tumour compression or direct invasion of the
oesophagus. Here we describe the case of an elderly female cement trader who
presented on account of complaints of difficulty in swallowing of three months
duration initially to solid foods and later to liquids. Chest x-ray done showed
a homogenous opacity in the left lower lung zone with obliteration of the left
costophrenic angle. Computed tomography scan revealed thickened left pleura
with reduced left lung volume. Upper gastrointestinal endoscopy revealed a
vague lower oesophageal stricture suggestive of metastatic cancer from a lung
primary. Patient had a gastrostomy on account of severe dysphagia. Her clinical
condition deteriorated during the third week of hospital admission. Despite
interventions and intensive care admission, she eventually succumbed to her
illness and was certified dead after 25 days of hospital admission. At autopsy,
there was a predominantly left-sided pleural-based mass with irregular
thickening of the pleura maximal at the costo-diaphragmatic region with nodular
involvement of the pericardium. Even though the oesophageal lumen was free of
tumour along its length, the closely related aorta was fixed to the vertebral
bones by tumour causing a mass effect. A conclusive diagnosis of epithelioid
mesothelioma of the left pleural was made based on the gross and microscopic
features of this tumour. This case suggests that in addition to recognized
risks among construction workers exposed to asbestos, cement sellers/traders
may also constitute an epidemiologic risk group for developing pleural
mesotheliomas. Large-scale population based prospective studies may be needed
to further explore this risk.
Keywords: pleural mesothelioma; dysphagia; cement trader
Introduction
Mesotheliomas are rare mesenchymal tumours that
arise from the neoplastic proliferation of mesothelial cells lining various
body cavities including the pleura, pericardium, peritoneum, and the tunica
vaginalis1. The majority of mesotheliomas arise in the
pleural cavity with a significant male predominance2.
The major risk factor for the development of mesothelioma is prolonged
occupational or environmental exposure to asbestos3. The
latency period from exposure to asbestos and the development of mesothelioma
ranges from 20 years to more than 40 years4. Dysphagia
is a rare, but recognised complication of advanced mesothelioma usually
occurring as a result of tumour compression or direct invasion of the
oesophagus5.
This case report highlights the unusual and rare
finding of dysphagia complicating pleural mesothelioma in an elderly female
cement trader. It also brings to fore the diagnostic dilemma and fatality that
can arise due to a low index of suspicion.
Case presentation
History and examination findings
The decedent was a
68-year-old nigerian female who presented at the university college hospital,
ibadan, nigeria on account of complaints of difficulty in swallowing of three
months duration. The difficulty in swallowing was initially to solid foods and then
gradually progressed to difficulty in taking liquids. There was associated
retrosternal chest pain and weight loss. There was no history of ingestion of
any corrosive substance. She is a known hypertensive. She did not take alcohol
or use tobacco in any form. She was a cement trader (who had been in the cement
trade for 20 years). Examination findings were those of a chronically
ill-looking elderly woman with significant chest findings of dull percussion
notes, and reduced breath sounds on the left lower lung zone. The remaining
physical examination was essentially normal.
Laboratory and radiologic investigations
Laboratory work-up
showed normal full blood count, urea, creatinine, and liver function tests.
However, there was hypokalaemia with serum k+ value of 2.0mmol/l (normal
reference range is 3.5-5.0mmol/l) and an elevated erythrocyte sedimentation
rate of 102 mm/hr (normal reference range is 0-15mm/hr.).
Chest x-ray done showed
a homogenous opacity in the left lower lung zone with obliteration of the left
costophrenic angle. The thoracic computed tomography (ct) scan revealed
thickened left pleura with reduced left lung volume. The oesophagus was dilated.
Upper gastrointestinal endoscopy revealed a vague lower third oesophageal
stricture suggestive of metastatic oesophageal malignancy from a lung primary
and a provisional diagnosis of an oesophageal malignancy was entertained.
However, the oesophageal biopsy done was negative for malignancy.
Clinical diagnosis, treatment and patient outcome
The patient then had a
gastrostomy on account of severe dysphagia. Her clinical condition deteriorated
around the third week of hospital admission. She developed marked dyspnoea and
subsequently had a cardiovascular arrest. Despite interventions and intensive
care admission, she eventually succumbed to her illness and was certified dead
after 25 days of hospital admission.
Autopsy findings
The significant
findings at autopsy were in the thoracic cavity. The left lung and visceral
pleura were morbidly adherent to the parietal pleural at the superior and
inferior aspects of the left hemithorax (figure 1a). There were areas of
pleural thickening and firm greyish-white tumour noted at the aforementioned
sites. The maximum thickness of the pleura is 1.1cm (at the costodiaphgragmatic
area, figure 1b). At the left lung apex, the tumour encompassed the
subclavian vessels. There were multiple tumour nodules seen at the pericardial
pleura ranging from 0.5cm to 1.5cm in diameter (figure 1c). The tumour
extended to the midline and involved segments of the thoracic aorta, firmly
attaching it to the vertebral bones. The
oesophagus; however, was free of tumour along its entire length (figure 1d).
There was atelectasis
of the left lung. The right lung was moderately heavy and weighed 650g
(reference range: 280-500g). The cut sections of the right lung showed moderate
oedema and congestion. 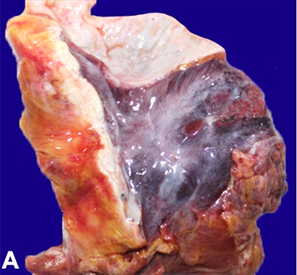
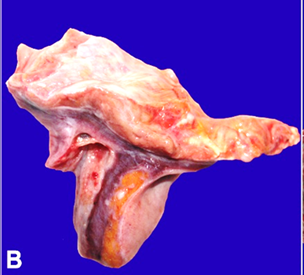
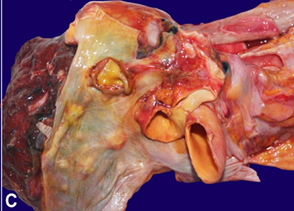

Figure 1. A - photomicrograph showing the inferior surface of the left lung
base (double green arrows). There is marked pleural thickening by greyish white
tumour (single green arrow).
B
- photomicrograph showing cut sections of the lung at the costophrenic angle
with markedly thickened pleural tissue (black arrows).
C
- pericardial surface with multiple greyish-white tumour nodules (black arrows).
D-
transverse section at the apical mediastinum showing greyish-white tumour
(single green arrow) infiltrating the posterior aspect of the aorta (double
green arrows). The oesophagus is located anteriorly (three green arrows) and it
is free from tumour involvement.
Definitive histopathologic diagnosis
The histologic
examination of the pleural mass showed a neoplasm composed of infiltrative
cells disposed in pseudo-acinar patterns. The tumour cells were relatively
monomorphic with bland nuclei and moderate amphophilic cytoplasm (figure 2a).
No cytoplasmic mucin vacuoles were seen. These tumour cells were seen to be
infiltrating the wall of the aorta (figure 2b). The underlying lung
tissue showed atelectatic changes. A conclusion of epithelioid mesothelioma of
the left pleural was made based on the gross and histologic features of this
tumour.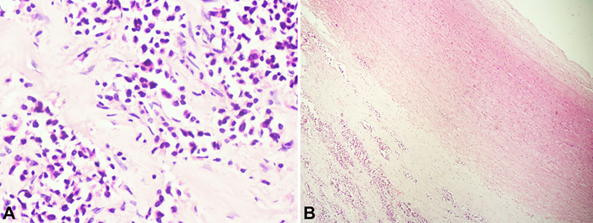
Figure 2. A: photomicrograph of the pleural tissue
showing infiltrative, mildly pleomorphic cuboidal cells disposed in
pseudoglandular patterns (hematoxylin and eosin stain, x 400 magnification).
B
- photomicrograph shows sections of the wall of the aorta with adventitial
infiltration by tumour cells (single black arrow). Double black arrows
highlight the tunica intima. (hematoxylin and eosin, x40).
Discussion
The decedent
presented primarily with symptoms of dysphagia which is a common presentation
of oesophageal disorders. Even though the chest imaging showed a lung mass, the
presenting symptom of dysphagia and findings of mild oesophageal stenosis in
the lower third initially was considered as indicative of oesophageal
involvement by a primary or metastatic lesion. The biopsies of the constricted
portion of the oesophagus were negative for malignancy, resulting in a clinical
diagnostic dilemma which could not be resolved until her demise.
At autopsy,
pleural-based masses involving the apical and costophrenic angle and the
pericardium were seen. The tumour had also encased and infiltrated the fibrous
wall of the large vessels (including the aorta and left subclavian vessels).
Regarding the aorta, the tumour caused an adherence of the aorta to the
vertebral wall. Interestingly, no evidence of direct oesophageal involvement by
the tumour was found. Nevertheless, the close anatomic relationship of the
aorta and the compressive mass effect on the oesophagus must have been
responsible for the difficulty in swallowing. Dysphagia is a rare but
recognized complication of advanced mesothelioma and this may be due to mass
effect of the tumour or direct infiltration into oesophageal lumen5.
Histologic
sections of the tumour showed features in keeping with mesothelioma.
Mesotheliomas can be histologically categorized into three main subgroups:
epithelioid type, sarcomatoid type and biphasic type (combining epithelioid and
sarcomatoid features).6 the epithelioid type is the most common subtype and it
shows epithelioid cells with ovoid-to-cuboidal nuclei with scanty to moderate
cytoplasm6.
The differential
diagnoses in this case were oesophageal malignancy and primary lung
adenocarcinoma. As earlier mentioned, the oesophageal mucosa was clean along
its entire length with no evidence of neoplastic involvement. The differential
diagnosis of primary lung cancer was also ruled out as the underlying lung
tissue only showed features of atelectasis. Also, the nuclear features typical
of adenocarcinomas such as eccentric or overlapping nuclei, vesicular
chromatin, nuclear pleomorphism, and cytoplasmic mucin vacuoles were lacking in
this case.4
Ancillary
investigations like immunohistochemistry can be helpful to further confirm this
diagnosis. Mesotheliomas are usually positive for calretinin, d2-40
(podoplanin) and wt1 while negative for epithelial markers such as ber-ep4 and
moc-317. These antibodies could not
be tested for because they are not readily available locally in a
resource-limited setting.
In this index
case, the significant risk factor identified appears to be prolonged exposure
to cement dust. In many developing countries such as nigeria, regulation of the
cement and asbestos content used in construction materials is limited. This has
resulted in continued use of adulterated cement, asbestos and other
construction materials with attendant health risks as seen in this case.
In spite of the
world health organization and international labour organization’s call for the
adoption of a program to eliminate asbestos-related disease among nations
through a ban on asbestos-containing materials, much is left to be seen in this
area in the west african sub-region8.
This case suggests
that in addition to recognized risks among construction workers exposed to
asbestos, cement sellers/traders may also constitute an epidemiologic risk
group for developing pleural mesotheliomas. Large-scale population based
prospective studies may be needed to further explore this risk.
Conclusion
This case
describes pleural mesothelioma presenting primarily with dysphagia in a
nigerian female cement trader and highlights the diagnostic challenges and
fatality involved when there is a low index of suspicion. It also brings to
bare the need for sustained public health policies, oversight and proper
regulation of the production, sale and use of cements, asbestos and other
constriction materials.
Declaration
Ethical approval and consent to participate
Not applicable
Consent for publication
Verbal and written consent was obtained from the deceased’s relatives to present the case for publication.
Availability of data and material
Not applicable.
Conflicts of interest
The authors have no conflict of interest to declare.
Funding
The authors did not receive any external funding in the course of writing and publishing this case report.
Author’s contribution
Authors idn and ooa performed the post-mortem examination. All authors reviewed the patient’s clinical records and autopsy findings and made the definitive histopathologic diagnosis. Authors idn and bla conceptualized the idea of presenting it as a case report. All authors participated in the writing and editing of the final manuscript.
Acknowledgement
Not applicable
References
1. hiriart e, deepe r, wessels a. Mesothelium and malignant
mesothelioma. J dev biol 2019;7(2):7.
2. delgermaa
v, takahashi k, park ek, le gv, hara t, sorahan t. Global mesothelioma deaths
reported to the world health organization between 1994 and 2008. Bull world
health organ 2011; 89(10):716-724.
3. neumann
v, löseke s, nowak d, herth fj, tannapfel a. Malignant pleural mesothelioma:
incidence, etiology, diagnosis, treatment, and occupational health. Dtsch
arztebl int 2013;110(18):319-326.
4. fels
elliott dr, jones kd. Diagnosis of mesothelioma. Surg pathol clin 2020;13(1):73-89.
5. santos
seoane sm, yano escudero r, arenas garcía v. An unexpected cause of dysphagia:
pleural mesothelioma. Rev esp enferm dig. 2019;111(6):494-495.
6. inai k. Pathology of mesothelioma. Environ health prev
med 2008; 13: 60-64.
7. chapel
db, schulte jj, husain an, krausz t. Application of immunohistochemistry in
diagnosis and management of malignant mesothelioma. Transl lung cancer res 2020;9(1):3-27.
8. moda hm., sawyerr h, clayson a. What will go wrong has
gone wrong: asbestos exposure risk among construction workers in nigeria.
Policy and practice in health and safety. 2018;16(2):212-223.