Relationship between Health Literacy and Physical Fitness of Japanese University Students
Abstract
Introduction: in recent years, attention has been focused on improving health literacy in a variety of settings. People with low health literacy do not practice various health behaviors including physical activity and are likely to be a group with high health risk. On the other hand, people with high health literacy practice various health behaviors and are expected to be physically active, which may lead to high physical function. The purpose of this study was to clarify the relationship between health literacy and physical fitness among college students.
Methods: eighty-two subjects who consented to the study were included in the study, and hls-eu-q47, ehealth, physical composition and physical fitness (10 m run, grip strength, yoyo test) were measured.
Results: in this study, there was no relationship between health literacy and physical fitness, but only between health literacy and physical fitness respectively (p < 0.05).
Conclusions: the reason why the relationship between health literacy and physical fitness was not found is thought to be due to the low level of health literacy among the japanese and the low utilization of health promotion and the lack of action to improve health.
Keywords: hls-eu-q47; ehealth; physical fitness; college student
1.
Introduction and contextualization
The ottawa charter of 1986 and the bangkok
charter of 2005 proposed a health strategy called health promotion for the
health of individuals and groups in society.
Health promotion is defined as "the
process of enabling people to control and improve their own health and its
determinants" and health literacy is positioned as one of its outcomes.
Health literacy has been defined in various
ways.
Cognitive social skills that determine an
individual's willingness and ability to access, understand, and use information
to promote and maintain good healt[1].
A variety of skills, including basic literacy
and numeracy, required in health care settings[2].
Degree of ability to obtain, organize, and
understand basic health information and services needed to make good health
decisions[3].
A broad range of skills and abilities
developed throughout life that enable people to find, understand, evaluate, and
use health information to reduce health risks and improve quality of life
through informed choices[4].
Important empowerment strategies that
increase people's ability to make good health decisions, control their own
health, find information, and take responsibility in their homes and
communities, in the workplace, in health care, in commerce, and in politics[5].
The knowledge, motivation, and ability to
obtain, understand, evaluate, and use health information so that they can make
decisions about health care, disease prevention, and health promotion in their
daily lives and maintain or improve their quality of life throughout their
lives[6].
Health literacy, as defined by the hls-eu
(european health literacy project), is simply the ability to make informed
decisions about health[6].
With the recent spread of the internet, the
concept of "information access" in health literacy should include not
only the ability to research but also the ability to select information
appropriately, and the ehealth literacy scale, which is limited to the internet
as a source of health information, has been developed. The ehealth literacy
scale (ehealth) was developed[7].
Ehealth is defined as "the ability to
search for, find, understand, and evaluate health information from electronic
sources, and to use the knowledge gained to solve health problems. Each
university has been improving the environment through various educational
methods and distinctive classes.
However, there have been no actual numerical
verifications of both objective and subjective indicators to measure this
effect, and there have been few similar reports.
The impact of low health literacy on health
and medical care includes: not using preventive services (flu shots and
mammograms), having less knowledge about diseases, treatments, and medications,
and dying 1.25 times earlier with insufficient health literacy than with sufficient
health literacy[8,9].
In addition, people with low health literacy
are less likely to practice a variety of health behaviors, including physical
activity, and are more likely to be at higher health risk, whereas individuals
with high health literacy practice a variety of health behaviors and are
expected to be physically active, and therefore may have high physical
functioning[10-13].
The purpose of this study was to clarify the
relationship between health literacy and physical fitness among college
students.
2.
Materials & methods/tables/graphs
About the subjects
Of the 629 participants who attended the
research orientation, 82 were included in the study after excluding those who
did not agree to participate in the study, those who were enrolled in more than
one course, and those who had not completed all data including the health
literacy and physical fitness survey tasks.
All participants were informed in writing and
verbally that participation in the study was voluntary, that their grades would
not be affected, and that they would not be disadvantaged if they withdrew.
This study was conducted with the approval of the research ethics committee of
momoyama gakuin university (approval number 29).
2.1
Health
literacy survey
The health literacy survey developed the
hls-eu-q47 (european health literacy survey questionnaire), which measures
acquisition, understanding, evaluation, and application (decision-making) in
the three domains of health care, disease prevention, and health promotion
using 47 questions questionnaire) was used[14].
We used a japanese translation of the
hls-eu-q47, which measures four competencies in health care, disease
prevention, and health promotion using 47 questions.
It measures the ability to obtain,
understand, evaluate, and use health information in the three domains of health
care, disease prevention, and health promotion. Responses to each question are
scored on a 4-point scale: very easy (4 points), somewhat easy (3 points),
somewhat difficult (2 points), and very difficult (1 point). Responses to each
question are scored on a 4-point scale.
Ehealth literacy is defined as the ability to
seek, find, understand, and evaluate health information from electronic sources
and to use the knowledge gained to solve health problems[7].
Ehealth score measures the ability to obtain,
understand, evaluate, and judge reliable health information on the internet as
ehealth score. The ehealth score measures the ability to obtain, understand,
evaluate, and judge reliable health information on the internet as the ehealth
score. The total score was calculated using the ehealth scale, a score
consisting of eight items (8-40 points) developed to measure the ability to
obtain, understand, evaluate, and judge reliable health information on the
internet.
The hls-eu-q47 and ehealth surveys were
administered using a web-based questionnaire (gooogle form).
Participants were given a paper copy of the
questionnaire regarding the purpose and application of the survey, as well as a
url with a qr code for their responses.
After responding, the qr-coded form was
collected and the responses on the form were matched to the responses on the
questionnaire. If there were any discrepancies in the responses, the paper
responses were adopted.
2.2
Physical
fitness surveys
Body composition (height, weight, body fat
percentage, fat mass, muscle mass*, muscle score), grip strength, 10 m run, and
yoyo test (intermittent recovery test: male level 2, female level 1) were
conducted.
Muscle mass was calculated for the right and
left arms, right and left legs, and trunk.
Grip strength and 10 m run were used as
indices of power, and yoyo test was used as an index of endurance (maximal
oxygen uptake).
Body composition was measured using the body
composition analyzer innerscan dual (rd-804l, tanita).
2.3
Yo-yo
intermittent recovery test (yo-yo irt)
The yo-yo intermittent recovery test (yo-yo
irt) is a repetitive exercise performed at gradually increasing speeds, with a
20-m round-trip sprint each way and a 10-second recovery time (jogging to a
marker located 5 m from the starting position and back) interspersed with
repetitions to a signal tone. The participants are asked to repeat the process
with a 10-second recovery period (jogging back and forth to a marker located 5
m from the starting position) in between. The interval between the signal tones
becomes shorter as the level increases, and failure is defined as failure to
return to the start line within the time limit. Failure is limited to two times
and is evaluated based on the distance traveled at the time of the second
failure. In this study, level 1 was used for females and level 2 for males.
2.4
Statistical
analysis
Correlations between hls-eu-q47, ehealth, 10-meter run, grip strength, and yoyo test were performed using pearson's product rate correlation coefficient (n = 82).
Ibm spss startistics 28 was used for all
statistical analyses, and the significance level of the tests was less than 5 %
(two-tailed).
3.
Results
& discussion
The results of the hls-eu-q47 showed that a higher percentage of our students answered "somewhat difficult" or "very difficult" compared to the 8 eu countries. This is similar to the results reported in 2015 for the general population in japan (1054 males and females aged 20-69), which showed that the health literacy of our students is low[15] (table 1).
Table 1. Percentages of “somewhat difficult” and very
difficult” in hls-eu-47 and comparison between eu, japan and our university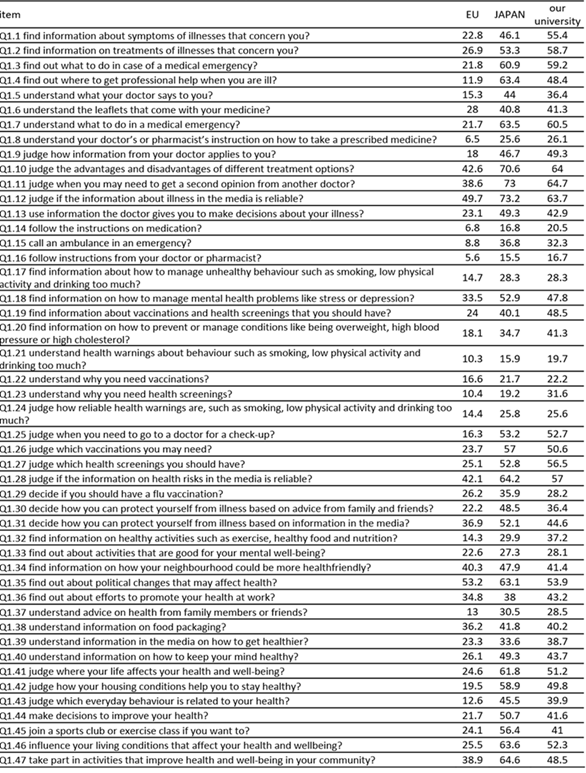
There was no relationship between ehealth,
the three domains of hls-eu-q47 (health care, disease prevention, and health
promotion) and physical fitness, but there was a relationship between
hls-eu-q47 and ehealth items related to health literacy and physical fitness
such as 10 m run and grip strength (table 2).
Table 2. Relationship between each measurement item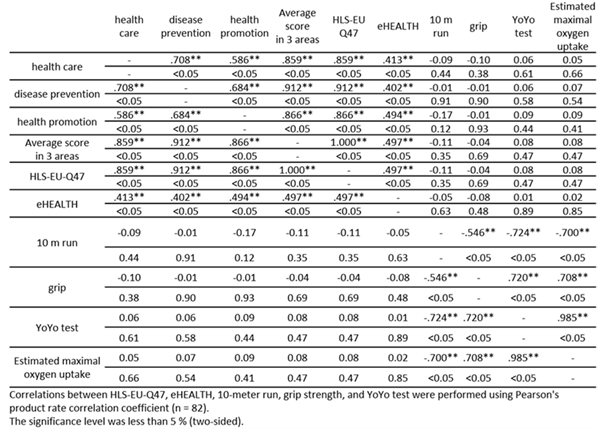
4.
Discussion
The hls-eu-q47 has been translated and
similar surveys have been conducted not only in japan but also in other asian
countries and regions[16]. The mean
scores of taiwan 34.4, malaysia 32.9, kazakhstan 31.6, indonesia 31.4, myanmar
31.3, and vietnam 29.6 were higher than those of our students (pre 28.03±6.88,
post 27.88±6.89).
However, the mean score of our students is
almost the same as that reported below for japanese students (table 3).
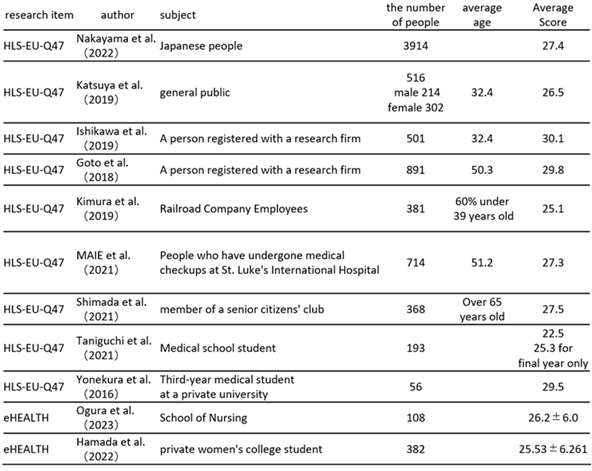
Thus, although the domestic surveys used
different methods and targets, such as web and questionnaire surveys, the
scores were all below 30, indicating that the average score of our students was
not low, but was about the same as the japanese average.
Similarly, ehealth reports were similar to
the results of our students (pre 24.18±5.74, post 25.37±6.37) (table 3).
Table 3. Subjects, ages and mean scores of health
literacy surveys conducted in japan.
Possible reasons for the lack of relationship
between physical fitness and health literacy are: 53.2% of the students in this
class aimed to improve their skills in exercise and other disciplines; compared
to the eu and other countries, their health literacy was low and they were not
able to obtain, understand and use information about physical activity and
health; the use of health promotion was low and they were not able to use
health promotion. Health promotion is low, and the respondents are not able to
take action to improve their health.
In this study, we investigated comparisons
and relationships among all subjects, but we have not yet conducted group
comparisons based on body composition. Although no relationship between
physical fitness and health literacy was found, it is possible that those with
high lean body mass (skeletal muscle mass) and adequate body fat mass are
predicted to have higher health awareness and behavior, and that a relationship
may be observed.
Conflict
of interest/ funding
This manuscript and similar manuscripts have
never been published in any language, except for abstracts and scholarly
articles, and there are no conflicts of interest or funding disclosures.
Ethical
approval
This study was approved by the research
ethics committee of momoyama gakuin university. Informed consent was obtained
from all participants before the study was conducted. Participants participated
in the study after paper forms and verbal explanations.
References
1.
Don
nutbeam. Health promotion glossary. Health promotion international.
1986;1(1):113-127.
2.
Ad hoc committee on health
literacy for the council. Jama 1999;281(6):552-557.
3.
U.s. Department of
health and human services. Health people 2010. Washington, dc: u.s. Government
printing office. 2000.
4.
Zarcadoolas
c, pleasant af, greer ds. Advancing health literacy: a framework for
understanding and action. Wiley 2006.
5.
Kickbusch i, maag d. Health
literacy. In: kris heggenhougen and stella quah, editors international
encyclopedia of public health 2008;3:204211.
6.
Sorensen
k, van den broucke s, pelikan jm, et al. Measuring health literacy in
populations: illuminating the design and development
process of the european
health literacy survey questionnaire (hls- eu-q). Bmc public health 2013;13:948.
7.
Norman cd, skinner ha. Eheals: the
ehealth literacy scale. J med internet res 2006;8(4):e27.
8.
Berkman nd, sheridan sl,
donahue ke, halpern dj, crotty k. Low health literacy and health outcomes: an
updated systematic review. Ann intern med 2011;155(2):97-107.
9.
David w baker, michael s wolf,
joseph feinglass, jason a thompson. Health literacy, cognitive abilities, and
mortality among elderly persons. J gen intern med 2008;23(6):723-726.
10.
Buja a, rabensteiner a,
sperotto m, et al. Health literacy and physical activity: a systematic review.
J phys act health 2020;17(12):1259-1274.
11.
Lim ml, van schooten ks,
radford ka, et al. Association between health literacy and physical activity in
older people: a systematic review and meta-analysis. Health promot int
2021;36(5):1482-1497.
12.
Matsushita
m, harada k, arao t. Relation between communicative and critical health
literacy and physical activity in japanese adults: across-sectional study. J
phys fit sports med 2018;7:75-80.
13.
Berkman nd, sheridan sl,
donahue ke, et al. Low health literacy and health outcomes: an updated
systematic review. Ann intern med 2011;155:97-107.
14.
Sørensen
k, van den broucke s, pelikan jm, et al. Measuring health literacy in
populations: illuminating the design and development process of the european
health literacy survey questionnaire (hls-eu-q). Bmc public health 2013;13:948.
15.
Nakayama
k, osaka w, togari t, et al. Comprehensive health literacy in japan is lower
than in europe: a validated japanese-language assessment of health literacy.
Bmc public health 2015;15:505.
16.
Duong
tv, aringazina a, baisunova g, et al. Measuring health literacy in asia:
validation of the hls-eu-q47 survey tool in six asian countries. J epidemiol
2017;27(2):80-86.