Safety of Cesarean Myomectomy: A Case Series from Sudan
Abstract
Background: uterine fibroids are benign tumors common among women of reproductive age. While cesarean myomectomy is often avoided due to potential complications, advances in surgical techniques and perioperative care have made it a viable option. This study evaluates the safety and outcomes of cesarean myomectomy, focusing on intraoperative, postoperative and reproductive outcomes among women in the red sea state, sudan.
Methods: a retrospective
study was conducted on 120 women who underwent cesarean myomectomy at port
sudan maternity hospital from 2014 to 2022. Demographic, clinical, obstetric
and perinatal data were collected and analyzed. Intraoperative and
postoperative outcomes, including blood loss, pain levels, hospital stay
duration and subsequent pregnancy rates, were assessed. Statistical analyses,
including logistic regression and chi-square tests, were used to identify
factors influencing these outcomes.
Results: the mean age of
the participants was 28 years, with the majority being primigravida. Each
patient had an average of 2 fibroids, with intramural fibroids being the most
common type (66.7%). Nearly all surgeries were completed with blood loss
between 250-500 ml and only one patient required a transfusion. No cases of
hysterectomy or surgical reopening occurred. Postoperative pain was mostly mild
(58.3%), with moderate pain reported by 41.7% of patients. Most patients
(64.2%) were discharged within two days and 60% of the participants
successfully conceived following the procedure. Logistic regression showed that
having multiple fibroid types or more than two fibroids increased the
likelihood of longer hospital stays, while chi-square tests revealed a significant
association between the number of fibroids and postoperative pain.
Conclusion:
cesarean myomectomy is a safe procedure with minimal complications and
favorable reproductive outcomes in appropriately selected patients. While
factors like fibroid number and type influence postoperative recovery and pain
levels, the procedure offers a viable option for managing fibroids during
cesarean delivery, reducing the need for future surgeries.
Keywords: myomectomy;
benign tumor; uterine fibroid; primigravida
Background
Uterine fibroids
(leiomyomas) are one of the most common benign tumors of the uterus and about
20-50% of women who are of reproductive age have them1,2. Particularly among black women, who are
more likely to report experiencing severe symptoms, as a result of various
environmental exposures and genetic variations3.
Fibroids are subdivided according to their location into subserosal, intramural
and submucosal. The size, quantity and location of the fibroids influence the
symptoms and available treatment options4.
Abnormal uterine bleeding, typically excessive menstrual bleeding, is the most
prevalent symptom. Pelvic pressure, bowel issues, frequent and urgent
urination, retention of urine, low back pain, constipation and dyspareunia are
other symptoms5,6.
The prevalence of uterine
fibroids in pregnancy was found to be about 16.7% in a recent study in cameroon7. Lower prevalence rates, such as 0.87% in
pakistan, were found in non-african populations8.
It is difficult to determine their precise incidence during pregnancy9. Nonetheless, a study indicates an
incidence of 3.9%, due to the increased vascularity of the gravid uterus, which
might result in excessive bleeding, unnecessary obstetric hysterectomy and
increased perioperative morbidity and mortality10.
Variable growth patterns
of the fibroids are influenced by hormonal and vascular changes during
gestation. While fibroids can increase the risks of complications such as
miscarriage, preterm birth, placenta previa, placental abruption and postpartum
hemorrhage, these effects depend on their size, number and location with
submucosal and multiple fibroids pose the highest risks11. Poor neonatal outcomes, such as low
5-minute apgar scores, which suggest a higher risk of newborn distress, have
also been associated with the presence of fibroids. While most pregnancies
reach term, risks include preterm delivery, low birth weight and increased
neonatal intensive care unit admissions. However, there were no neonatal
deaths, suggesting fair overall perinatal outcomes despite higher risks
associated with fibroids12.
In general, symptomatic
fibroids should be detected early for optimal treatment, given the prevalence
of intramural fibroids in sudanese women. It is advised to conduct additional
imaging methods like mri to have a better understanding of the anatomical distribution
of uterine fibroids13. Close
observation and a high degree of suspicion regarding possible problems are
necessary for the management of pregnancies affected by fibroids to prevent its
complications14.
Cesarean myomectomy is a
surgical procedure where fibroids are being removed during the cesarean
section. It is considered complex and it is usually avoided due to the
potential increase in blood loss, infection, uterine rupture and other
complications. It has been a topic of considerable debate, with differing
opinions on whether it should be considered a feasible and safe procedure or an
absolute contraindication, growing evidence now supports its safety in
carefully selected cases15.
Moreover, obstetricians increasingly choose to perform myomectomy during the
cesarean section in modern obstetrics due to improvements in anesthesia,
sufficient blood product availability, selective devascularization techniques
and a multidisciplinary approach. This saves the patient from future morbidity
caused by multiple surgeries, anesthetic complications and out-of-pocket
expenses16.
This study aims to
evaluate the safety and the nature of intraoperative and postoperative outcomes
associated with cesarean myomectomy among women in the red sea state, sudan.
Methods and materials
This was a retrospective case series study with
longitudinal follow-up for short and long term outcomes post cesarean
myomectomy. We report a total of 120 patients with their demographic, clinical
and obstetric data as well as perinatal outcomes. The study was conducted at
port sudan maternity hospital, red sea state, sudan. Which is the largest
hospital in the region to provide maternal healthcare services and it is
considered a referral center for all complicated cases in the eastern part of
sudan.
Data was collected from the records over eight years
(2014–2022), included records of pregnant women with uterine fibroids who
underwent cesarean myomectomy during cesarean section after providing informed
consent following detailed counseling on the procedure's potential risks and
benefits, with data collected on estimated blood loss, risk of intraoperative
bleeding, need for blood transfusion, risk of peripartum hysterectomy, hospital
stay duration and postoperative pain.
Data management and analysis
Data were collected using a structured google forms
questionnaire and then transferred to excel for initial cleaning and coding.
The coded dataset was subsequently imported into ibm spss statistics version 23
for analysis. Descriptive statistics summarized demographic and clinical
variables, with means and standard deviations for continuous data and
frequencies with percentages for categorical data. Results were presented in
tables for clarity. Direct logistic regression assessed associations between
predictors (age, fibroid number/type, parity) and two outcomes: postoperative
hospital stays duration and pregnancy rate. Chi-square tests evaluated
relationships between pain levels and fibroid characteristics, with cramer’s v
indicating effect size where applicable. Analyses used a 95% confidence level,
with significance set at p < 0.05.
Ethical considerations
Ethical approval was granted by the red sea state
ministry of health ethical committee and the local research committee at port
sudan maternity hospital, red sea state, sudan. Permissions from the hospital
management were also obtained from the general manager and the medical
director. Patients' data was secured and anonymized using serial numbers to
protect confidentiality and privacy. Identifiable information was removed and
all analyses were conducted on de-identified datasets, ensuring compliance with
ethical standards and relevant data protection regulations. The data were
exclusively used for research purposes in adherence to these guidelines.
Description of the procedure
A low transverse or vertical uterine incision is made
depending on the location of the fibroids, followed by the delivery of the baby
and complete removal of the placenta and membranes. After delivery, fibroids,
typically subserosal or intramural, are visually identified and addressed. A
direct incision is made over the fibroid using a scalpel or electrosurgical
device and techniques such as the use of a tourniquet or vasopressin are
employed to minimize blood loss. When a tourniquet is used, an on-and-off technique
is applied to mitigate the risk of uterine atony after its removal. For cases
involving multiple uterine fibroids, efforts are made to minimize incisions by
removing multiple fibroids through a single incision. The fibroid is carefully
dissected from the surrounding myometrium, with any adhesions released.
Bleeding vessels are clamped, sutured or cauterized and uterotonic agents, such
as oxytocin, are administered to promote uterine contraction and reduce
hemorrhage. The myometrial defect is repaired in multiple layers using
absorbable sutures (vicryl size 2) to ensure uterine integrity and reduce the
risk of uterine rupture in subsequent pregnancies, with the serosa closed using
vicryl size 2-0 or 3-0. The uterine incision made for delivery is sutured in
layers and the abdominal wall is closed in the standard manner. A surgical
drain is routinely placed for 24 hours to monitor blood loss. Postoperatively,
the patient is closely monitored for complications such as postpartum
hemorrhage, infection or thromboembolic events, with pain management, early
mobilization and administration of uterotonic medications provided as part of
routine care. In general cesarean myomectomy can be done for all types of
fibroids, weather submucosal, intramural, subserosal or mixed type (figure
1).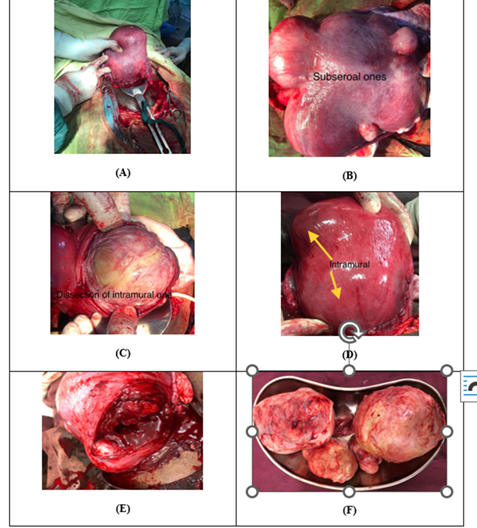
Figure
1:
Pictures of Different Fibroid Types Following Cesarean Myomectomy: Subserosal
type are shown as single (A) and multiple (B). Intramural type shown in (C) and
(D). Mixed with all types of fibroids are presented in one patient shown in (E)
and (F).
RESULTS
Demographics
Our study included a total of 120 women who
underwent cesarean myomectomy at Portsudan Maternity Hospital during the study
period (2014 - 2022). The mean age of patients was 28.02 ± 4.27 years, ranging
from 20 to 35 years. All the patients were married with a mean duration of
marriage of 3.58 ± 2.14 years and the majority were primigravida (50.8%, N =
61), while the remaining (49.2%, N = 59) had experienced one or more previous
pregnancies. (Table 1).
Table 1: Patient demographic and clinical characteristics
|
|
Mean |
SD |
Range |
Frequency |
Percentage % |
|
|||||
|
|
Age
(years) |
28.02 |
4.268 |
20 - 35 |
|
|
|||||
|
|
Marriage
duration (years) |
3.58 |
2.141 |
1 - 8 |
|||||||
|
|
Gravidity |
||||||||||
|
|
Primigravida |
61 |
50.8 % |
||||||||
|
|
Para 1 |
34 |
28.3 % |
||||||||
|
|
Para 2 |
15 |
12.5 % |
||||||||
|
|
Para 3 |
7 |
5.8 % |
||||||||
|
|
Para 4 |
3 |
2.5 % |
||||||||
The number of fibroids per patient ranged from
1 to 4, with an average of 2.04 ± 0.85. (Table 2) Intramural fibroids were the
most common type, affecting 66.7% of the patients (N = 80), while sub-mucosal
fibroids were the least common. A small subset of patients (6.7%, N = 8) had
multiple fibroid types, while the majority (93.3%, N = 112) had only one type.
Intraoperative and postoperative outcomes
During the surgeries, the average
intraoperative blood loss for the vast majority of patients (99.2%, N= 119) was
250 - 500 mL. Only one patient (0.8%) required a blood transfusion due to
excessive intraoperative blood loss of more than 500 ml. However, none of our
120 patients required hysterectomy nor reopening following the procedure.
All the surgical procedures had a duration
ranging from 30 to 60 minutes. Postoperatively, the length of hospital stay
varied between 1 and 4 days, with 64.2% (N = 77) of patients staying for 1–2
days and 35.8% (N = 43) staying for 3-4 days. (Table 2).
Table 2: Fibroid characteristics
|
Mean |
SD |
Range |
Frequency |
Percentage % |
|
||
|
2.03 |
0.855 |
1 - 4 |
|
|
|
||
|
Type of
fibroid |
|||||||
|
Submucosal |
21 |
17.5% |
|||||
|
Intramural |
80 |
66.7% |
|||||
|
Subserosal |
27 |
22.5% |
|||||
Most patients reported mild pain following the
procedure (58.3%, N = 70), while 41.7% (N = 50) reported moderate pain and none
reported severe pain (0%, N = 0).
More than half of patients got pregnant
following the procedure (60%, N = 72).
Statistical Assessment of Surgical Outcomes and
Pain
Direct logistic regression was performed to
assess the impact of a set of factors on the duration of post-operative
admission. The model contained a set of independent variables (age, number of
fibroids, type of fibroid and number of parity). The strongest predictor for a
longer duration of post-operative admission was having two types of fibroids
with an odds ratio of 9.2. An increased number of fibroids was also associated
with a higher likelihood of a longer post-operative admission (Odds ratio (OR) =
1.385 for 2 fibroids and OR = 1.789 for 3 or more fibroids).
However, the overall model, containing all
predictors, was statistically insignificant, χ2 (9, N = 120) = 9.99, p = 0.351,
indicating that the full model was not able to reliably distinguish between
patients based on their post-operative admission duration. (Table 3).
Table 3: Logistic regression predicting the duration of
post-operative admission
|
|
B |
S.E |
Odds Ratio |
95% CI for Odds Ratio |
P-value |
|
|
Lower |
Upper |
|||||
|
Age |
-.073 |
0.055 |
0.93 |
0.835 |
1.036 |
0.188 |
|
Number of fibroids
One |
|
|
|
|
|
0.621 |
|
Two |
0.325 |
0.497 |
1.385 |
0.523 |
3.666 |
0.512 |
|
Three
or more |
0.582 |
0.608 |
1.789 |
0.543 |
5.896 |
0.339 |
|
Type of fibroid
Submucosal
|
|
|
|
|
|
0.237 |
|
Intramural |
0.819 |
0.699 |
2.268 |
0.576 |
8.922 |
0.241 |
|
Subserosal |
0.611 |
0.790 |
1.843 |
0.392 |
8.667 |
0.439 |
|
Two types |
2.220 |
1.104 |
9.204 |
1.058 |
80.064 |
0.044 |
|
Number of
parity
Zero |
|
|
|
|
|
0.822 |
|
One |
0.051 |
0.483 |
1.052 |
0.408 |
2.713 |
0.916 |
|
Two |
-0.355 |
0.706 |
0.701 |
0.176 |
2.800 |
0.615 |
|
Three or
more |
0.539 |
0.816 |
1.713 |
0.346 |
8.488 |
0.509 |
Another Direct logistic regression was
performed to assess the impact of the same factors on the rate of pregnancy
after 1st surgery. Having only intramural or subserosal fibroids was linked to
less likelihood of pregnancy after surgery (OR = 0.145 or = 0.112
respectively). However, the full model containing all predictors was
statistically insignificant, χ2 (9, N = 120) = 16.183, p = .063, indicating
that the model was not able to reliably predict the rate of pregnancy based on
these factors. (Table 4).
Table 4: Logistic regression predicting the rate of pregnancy after 1st surgery
|
|
B |
S.E |
Odds
Ratio |
95% CI
for Odds Ratio |
P-value |
|
|
Lower |
Upper |
|||||
|
Age |
0.090 |
0.055 |
1.094 |
0.981 |
1.219 |
0.106 |
|
Number of fibroids
One |
|
|
|
|
|
0.664 |
|
Two |
0.445 |
0.492 |
1.560 |
0.595 |
4.091 |
0.366 |
|
Three or more |
0.276 |
0.610 |
1.318 |
0.399 |
4.354 |
0.650 |
|
Type of
fibroid
Submucosal
|
|
|
|
|
|
0.064 |
|
Intramural |
-1.903 |
0.838 |
0.149 |
0.029 |
0.772 |
0.023 |
|
Subserosal |
-2.193 |
0.905 |
0.112 |
0.019 |
0.658 |
0.015 |
|
Two
types |
-0.808 |
1.230 |
0.446 |
0.040 |
4.965 |
0.511 |
|
Number of parity
Zero |
|
|
|
|
|
0.280 |
|
One |
0.957 |
0.508 |
2.603 |
0.961 |
7.050 |
0.060 |
|
Two |
0.707 |
0.674 |
2.028 |
0.541 |
7.596 |
0.294 |
|
Three or more |
0.591 |
0.838 |
1.805 |
0.350 |
9.324 |
0.481 |
A chi-square test of independence was performed
to examine the association between post-operative pain levels (mild vs.
moderate) and two independent variables: the number of fibroids and the type of
fibroids. (Table 5).
Table 5: Crosstabulation for post-operative pain level
and fibroid characteristics
|
|
Post-operative pain |
Total |
||
|
Mild |
Moderate |
|||
|
Number of fibroids |
One |
27 (71.1%) |
11 (28.9%) |
38 (100%) |
|
Two |
28 (62.2%) |
17 (37.8%) |
45 (100%) |
|
|
Three or more |
15 (40.5%) |
22 (59.5%) |
37 (100%) |
|
Post-operative pain level and number of
fibroids
There was a statistically significant
association between post-operative pain level and the number of fibroids, χ²
(2, N = 120) = 7.629, p = 0.022, Cramer’s V = 0.252. Patients with three or
more fibroids were significantly more likely to report moderate post-operative
pain compared to those with fewer fibroids.
Post-operative pain level and type of fibroid:
Patients with subserosal fibroids were more
likely to experience moderate post-operative pain, while those with submucosal
fibroids tended to report mild pain. However, the chi-square test was not
statistically significant, χ² (2, N = 120) = 3.958, p = 0.138, Cramer’s V =
0.188.
Discussion
Our
study examined the intraoperative and postoperative outcomes of cesarean
myomectomy involved 120 women at Port Sudan Maternity Hospital, in the period
from 2008 to 2022. Our findings demonstrate a generally favorable profile for
cesarean myomectomy, with minimal intraoperative complications, manageable
postoperative pain levels and promising fertility outcomes17,18. Demographic data indicates that the
majority of patients were young (mean age 28.02 years), primarily primigravida
and underwent surgery with an average of two fibroids, predominantly
intramural. In our study, more than half of the participants were nulliparous
(50.8%), indicating a significant proportion of first-time mothers undergoing
cesarean myomectomy. This finding aligns with the results reported by Ramya et
al, who also observed a predominance of nulliparous women in their study
population (70%)19. Similarly,
Kanthi et al. highlighted the occurrence of cesarean myomectomy in nulliparous
women, emphasizing the importance of careful surgical planning in this group
due to their desire for future fertility20.
This may be attributed to hormonal fluctuations and a decreased responsiveness
of leiomyomas to estrogen receptors21,22.
Another
explanation for higher prevalence of nulliparous women undergoing cesarean
myomectomy could reflect their increased likelihood of presenting with
symptomatic fibroids during their first pregnancy, as well as the tendency for
physicians to address these fibroids during cesarean delivery to prevent future
complications23.
Intraoperatively,
blood loss remained within acceptable limits (250-500 mL for 99.2% of patients)
and none required a hysterectomy or surgical reopening, indicating a low risk
profile for this procedure. Notably, only one patient (0.8%) required a blood transfusion
due to intraoperative blood loss exceeding 500 mL. This finding aligns with the
results reported by Ramya et al, who also observed that cesarean myomectomy
could be conducted without the need for blood transfusions in the majority of
cases24. The low incidence of
significant bleeding in our study can be attributed to careful surgical
techniques, improved anesthesia protocols and the availability of blood
products and advanced hemostatic measures. Moreover, the increased vascularity
of the gravid uterus, traditionally viewed as a deterrent to performing
myomectomy during cesarean section, can be effectively managed with modern surgical
tools and a multidisciplinary approach25,26.
The reduced intraoperative complication rates in this study underscore the
importance of careful patient assessment and surgical precision in minimizing
risks27. Postoperative recovery,
reflected in hospital stays and pain levels, was manageable for most patients.
The majority had short hospital stays (1-2 days) and reported mild pain.
Statistical analysis revealed a significant association between the number of
fibroids and pain level, with those having three or more fibroids more likely
to experience moderate pain. The absence of severe pain reports further
emphasizes the procedure’s tolerability, though pain management may need closer
attention for patients with multiple fibroids28,29.
Fertility outcomes are of particular relevance, given the patient population's
profile and reproductive goals. The study found that 60% of patients achieved
pregnancy within 1-2 years post-surgery, suggesting that cesarean myomectomy
can support future fertility. However, the logistic regression analysis
revealed that intramural and subserosal fibroids were associated with a lower
likelihood of pregnancy, highlighting the potential impact of fibroid type on
fertility outcomes30. Despite the
valuable insights, this study had limitations, including its single-center
design and the lack of a comparative group of cesarean deliveries without
myomectomy. Further research across multiple centers could validate these
findings and provide a broader understanding of cesarean myomectomy's impact on
fertility and recovery outcomes.
Conclusion
Cesarean
myomectomy is a safe and effective option for addressing fibroids in women
desiring fertility preservation, challenging the traditional preference for
interval myomectomy. With proper patient selection, preoperative planning and
the involvement of trained and experienced surgeons, it offers favorable
intraoperative and postoperative outcomes, reduces the need for additional
surgeries and supports reproductive health. The findings advocate for revising
clinical guidelines to integrate cesarean myomectomy into routine practice,
emphasizing the importance of specialized training to ensure safety and
success. This is particularly crucial in resource-limited settings, where
access to advanced surgical care is restricted. Future research should focus on
refining techniques and patient selection criteria to further optimize
outcomes, solidifying cesarean myomectomy as a valuable advancement in
obstetric surgery.
References
1. Senturk
MB, Polat M, Doǧan O, Pulatoǧlu Ç, Yardlmcl OD, Karakuś R, et al. Outcome of
Cesarean Myomectomy: Is it a Safe Procedure? Geburtshilfe Frauenheilkd
2017;77:1200-1206.
2. Sarwar
I, Habib S, Bibi A, Malik N, Parveen Z. Clinical audit of foetomaternal outcome
in pregnancies with fibroid uterus. J Ayub Med Coll Abbottabad 2012;24:79-82.
3. http://dx.doi.org/10.1016/j.earlhumdev.2015.09.003%5Cnhttp://dx.doi.org/10.1016/j.earlhumdev.2014.01.002%5Cnhttp://dx.doi.org/10.1016/S0378-3782(12)70006-3%5Cnhttp://www.sciencedirect.com/science/article/pii/S2341287914000763%5Cnhttp://dx.doi.org/10.1016/
4. Wallach
EE, Vlahos NF. Uterine myomas: An overview of development, clinical features
and management. Obstet Gynecol 2004;104:393-406.
5. Anderson
DE. Diagnosis and Management of Uterine Torsion. Vet Tech Llamas Alpacas,
Second Ed 2023;247-251.
6. Stewart
EA, Cookson CL, Gandolfo RA, Schulze-Rath R. Epidemiology of uterine fibroids:
a systematic review. BJOG An Int J Obstet Gynaecol 2017;124(10):1501-1512.
7. Egbe
TO, Badjang TG, Tchounzou R, Egbe EN, Ngowe MN. Uterine fibroids in pregnancy:
Prevalence, clinical presentation, associated factors and outcomes at the Limbe
and Buea Regional Hospitals, Cameroon: A cross-sectional study. BMC Res Notes
2018;11:4-9.
8. Choudhary
A, Inamdar SA, Sharma U. Pregnancy with Uterine Fibroids: Obstetric Outcome at
a Tertiary Care Hospital of Central India. Cureus 2023;15:5-7.
9. Hartmann
KE, Laughlin SK, Baird DD, Savitz DA, Herring AH. Prevalence of uterine
leiomyomas in the first trimester of pregnancy: An ultrasound-screening study.
Obstet Gynecol 2009;113:630-635.
10. Lolis
DE, Kalantaridou SN, Makrydimas G, Sotiriadis A, Navrozoglou I, Zikopoulos K,
et al. Successful myomectomy during pregnancy. Hum Reprod 2003;18:1699-1702.
11. Coutinho
LM, Assis WA, Spagnuolo-Souza A, Reis FM. Uterine Fibroids and Pregnancy: How
Do They Affect Each Other? Reprod Sci 2022;29:2145-2151.
12. Radhika
BH, Naik K, Shreelatha S, Vana H. Case series: Pregnancy outcome in patients
with uterine fibroids. J Clin Diagnostic Res 2015;9:01-04.
13. Abdelmtalab
MAA, Tahir O, Hussein K, Badawi K. Anatomical locations of uterine fibroids in
Sudanese women. Anat J Africa 2020;9:1701-1706.
14. Giuliani E, As-Sanie S, Marsh EE. Epidemiology
and management of uterine fibroids. Int J Gynecol Obstet 2020;149:3-9.
15. Goyal
M, Dawood AS, Elbohoty SB, Abbas AM, Singh P, Melana N, et al. Cesarean
myomectomy in the last ten years; A true shift from contraindication to
indication: A systematic review and meta-analysis. Eur J Obstet Gynecol Reprod
Biol 2021;256:145-157.
16. Kathpalia
SK, Arora D, Vasudeva S, Singh S. Myomectomy at cesarean section: A safe
option. Med J Armed Forces India 2016;72:161-163.
17. Garg
P, Bansal R. Cesarean myomectomy: a case report and review of the literature. J
Med Case Rep 2021;15:1-4.
18. Akinajo
OR, Ugwu AO, Ezenwankwo FC, Soibi-Harry AP. Multiple uterine fibroids in an
18-year-old: a case report and review of literature. South Sudan Med J 2020;13:156-159.
19. Kakade
A, Wagh G. Evaluate the Feasibility of Surgical Transversus Abdominis Plane
Block for Postoperative Analgesia After Cesarean Section. J Obstet Gynecol
India 2019;69:330-333.
20. Kanthi
JM, Sumathy S, Sreedhar S, Rajammal B, Usha MG, Sheejamol VS. Comparative Study
of Cesarean Myomectomy with Abdominal Myomectomy in Terms of Blood Loss in
Single Fibroid. J Obstet Gynecol India 2016;66:287-291.
21. Lauren
A. Wise, Julie R. Palmer, Bernard L. Harlow, Donna Spiegelman, Elizabeth A.
Stewart, Lucile L. Adams-Campbell LR. Reproductive Factors, Hormonal
Contraception and Risk of Uterine Leiomyomata in African-American Women: A
Prospective Study. Am J Epidemiol 2004.
22. Sparić R andrić L, Guler O, Malvasi A, Babović I,
Hatirnaz S, et al. Cesarean Myomectomy: Reflections on
Clinical and Surgical Controversies between a New Trans-Decidual Technique vs.
Traditional Method. Med 2024;60.
23. Sparić
R, Kadija S, Stefanović A, Spremović Radjenović S, Likić Ladjević I, Popović J,
et al. Cesarean myomectomy in modern obstetrics: More light and fewer shadows.
J Obstet Gynaecol Res 2017;43(5):798-804.
24. Ramya
T, Sabnis SS, Chitra TV, Panicker S. Cesarean Myomectomy: An Experience from a
Tertiary Care Teaching Hospital. J Obstet Gynecol India 2019;69:426-30.
25. Umezurike
C, Feyi-Waboso P. Successful myomectomy during pregnancy: A case report. Reprod
Health 2005;2:2003-2005.
26. Ghaemmaghami F, Karimi-Zarchi M, et al. Successful
Myomectomy during Cesarean Section: Case report Literature Review. Int J Biomed
Sci 2017;13:110-112.
27. Chauhan
AR. Cesarean Myomectomy: Necessity or Opportunity? J Obstet Gynecol India 2018;68:432-436.
28. Mishra
S, Sinha N, Prasad A, Kumar A. A case report on caesarean myomectomy. Int J
Reprod Contraception Obstet Gynecol 2024;13:1337-1340.
29. Guler
AE, Guler ZÇD, Kinci MF, Mungan MT. Myomectomy During Cesarean Section: Why Do
We Abstain From? J Obstet Gynecol India 2020;70:133-137.
30. Zhao
R, Wang X, Zou L, Zhang W. Outcomes of Myomectomy at the Time of Cesarean
Section among Pregnant Women with Uterine Fibroids: A Retrospective Cohort
Study. Biomed Res Int 2019.