Scrofuloderma Case Report
ABSTRACT
Scrofuloderma is the most common clinical type of chronic subcutaneous
tuberculosis in our environment. It is mainly caused by Mycobacterium
tuberculosis, which is characterized by producing cold abscesses and secondary
liquefaction of the adjacent skin; this results in scrofuloderma: a cutaneous
lesion that covers another tuberculous process, frequently lymphadenopathy.
Furthermore, scrofuloderma manifests itself with frequent fistulization, which
can last for months or years, if an accurate and timely diagnosis and treatment
are not carried out, it may remit and go unnoticed by the patient or health
personnel. Hereby we present the case of a patient with scrofuloderma treated
in our hospital unit.
Keywords: Scrofuloderma; Cutaneous TB; Tuberculosis;
Extrapulmonary TB
INTRODUCTION
Cutaneous Tuberculosis represents less than 2% of all cases reported by
M. Tuberculosis. Scrofuloderma and Lupus vulgaris are the most common clinical
forms of cutaneous TB worldwide; this is associated with a moderate resistance
of the body's innate immunity and is a chronic condition; It is caused mainly
by M. tuberculosis variety Hominis, and to a lesser extent by M. Bovis1,2. It can affect any group age, with higher
prevalence in children, young adults and elderly3.
The present case report is of clinical importance as being a pathology
of chronic evolution, it can go unnoticed, or underdiagnosed in inexperienced
clinical eyes, and it is usually treated as a simple bacterial abscess
recurrently, and without adequate follow-up. clinical. This clinical case has
presented informed consent for the publication of its content and iconography,
maintaining confidentiality.
PRESENTATION OF THE CLINICAL CASE
We present the case of a 25-year-old female patient, born in the
Province of Cotopaxi and resident in the City of Quito, Ecuador. She did not
have comorbidities or significant family medical history. She reported a right
supraclavicular cutaneous abscess for 5 years, which was drained without any
complications; she did not have any extension studies (Figure 1). 
Figure 1. Histopathology
of the cervical lymph node with HE staining shows multiple granulomas of
different sizes with a nodular arrangement. Courtesy of Dr. Pedro León,
pathologist.
Three months ago she presented a right subclavicular mass which was
treated as a recurrent soft tissue bacterial abscess by medical personnel on
several occasions; she received multiple antibiotic regimens, without
improvement. On physical examination, we noted a 4-cm erythematoviolaceous
rubbery plaque, slightly painful, with occasional serohematic fluid leakage, as
well as surrounding longitudinal scars. Furthermore, she presented a painful 1
cm lymph node in the right axilla (Figure
2). 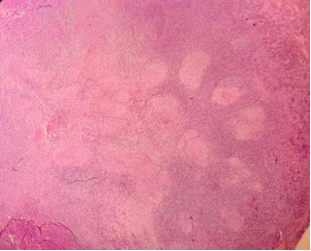
Figure 2. With a higher
magnification lens, epithelioid histiocyte granulomas with the presence of
multinucleated giant cells are evident. Courtesy of Dr. Pedro León, pathologist.
Among the important laboratory and imaging examinations, A chest x-ray
reported multiple microcalcifications throughout the lung field; In addition, a
soft tissue ultrasound was performed demonstrating a soft tissue mass of 29 x 6
x 18 mm with a volume of 1.7 ml, and the Doppler showed increased vascularity
in relation to an abscess in formation, along with 2 thickened lymph nodes of 6
and 17 mm. A rapid TB detection test (GeneXpert MTB/RIF ULTRA) of a thoracic
and axillary lymph node biopsy turned reactive (Figure 3).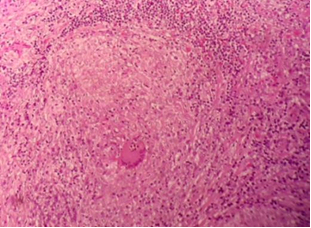
Figure 3. Ziehl Neelsen
stain identifies rods that are morphologically compatible with acid-fast
bacilli (arrow). Courtesy of Dr. Pedro León, pathologist.
A simple chest tomography showed an increase in the size of the
cervical, supraclavicular, subclavicular and bilateral axillary lymph nodes; No
pathological changes were identified at the lung level.
Given the clinical diagnosis and positive PCR for cutaneous TB, a
Isoniazid, rifamping, pyrazinamide, ethambutol anti-tuberculosis regime was
started, after one month of monitoring the patient with improvement in clinical
evolution.
The histology result of the lymph node shows multiple granulomas of
different sizes with a nodular arrangement characterized by epithelioid
histiocytes with the presence of multinucleated giant cells of Langerhans-type
morphology and occasional central necrosis; With Ziehl Neelsen staining,
occasional rods morphologically compatible with acid-fast bacilli compatible
with lymph node tuberculosis were identified.
There were no clinical criteria to initiate isoniazid preventive
treatment (IPT) for the patient's close contacts.
DISCUSSION
In Ecuador during 2021, there is a report of a total of 6,330 new cases
of TB, of which 5,973 patients presented tuberculosis and 357 cases of
drug-resistant tuberculosis4. The
incidence rate of tuberculosis in Ecuador in that year was 48 for every 100,000
person5,6. During 2018, extrapulmonary
TB cases constituted 18.46% of total TB cases7.
Within the clinical presentation,
scrofuloderma manifests as an indurated erythematous-violet nodule or gum on
the skin, which is covered by another tuberculous process (infection due to
contiguity, although it can also occur due to systemic contamination), usually
from a lymph node. There are other locations from which the nodule can extend
such as pleura, abdomen, tract genitourinary, joints, bones and meninge1,2. The nodule
or gum progressively grows, abscesses and then opens to the outside through
fistulas that release serous, purulent or caseous material, producing
induration of the adjacent skin area, nodules, gummas and cold abscesses; Very
frequently it heals and involutes, repeating the cycle every certain period of
time, leaving scars8,9. The most
frequently affected places are the neck, chest wall, armpits and inguinal
region1.
The current recommendation according to the WHO is the use of an
automated PCR test such as the GeneXpert® MTB/RIF ULTRA as an initial test for
the diagnosis of pulmonary or extrapulmonary TB and/or MDR-TB, which is
obtained in two hours10. The Gold
standard test for diagnosis remains bacteriological examination by tissue
culture or biopsy. Other tests of great diagnostic value are the observation of
bacilli using Ziehl Neelsen staining8,9.
The standard antifungal treatment for cutaneous tuberculosis in Ecuador
is the same as in the pulmonary forms, which consists of an initial phase of
four drugs isoniazid, rifampicin, pyrazinamide and ethambutol (2HRZE), for two
months, followed by the consolidation phase of four months of use of isoniazid
and rifampicin (4HR).
CONCLUSIONS
Scrofuloderma, like the rest of cutaneous TB, is a rare entity that can
go unnoticed by the patient or due to a lack of expertise on the part of the
healthcare professional, since it is a slowly evolving pathology and can often
be found latent, until moment that triggers symptoms and puts the patient on
alert, in which case he underwent multiple antibiotic treatment regimens
without resolution and relapsed twice in a period of 5 years. The patient did
not report pulmonary symptoms or having had close contact or being in
overcrowded conditions. There is no doubt that active surveillance must be
carried out in cases of cutaneous TB to make an accurate and timely diagnosis,
avoiding unnecessary treatments due to the lack of diagnostic suspicion.
REFERENCES
1. Ruiz-Márquez EA, Navarrete-Solís J,
González-Cabello D. Scrofuloderma: Case report. Cosomotic, Medical and Surgical Dermatology 2020;18(1):28-30.
2. Franco-Paredes C, Marcos LA,
Henao-Martínez AF, et al. Cutaneous mycobacterial infections. Clin microbiol Rev 2018;32(1).
3. Concha M, Fich F, Rabagliati R, et
al. Tuberculosis cutánea: reporte de dos casos y revisión de la
literatura. Rev Chile Infect 2011;28(3):262-268.
4. de Brito Vieite CMA. Health and Environment Ranking: A study
of the countries at the iberoamerican region and its challenges ahead. RISUS 2019;10(1):143-152.
5. Silva G, Perez F, Marín, D. Tuberculosis en niños y adolescentes
en Ecuador: análisis de la notificación, las características de la enfermedad y
el resultado del tratamiento. Rev
Panam Salud Publica 2019;43.
6. Cantos YYQ, Choez AAL, Andrade PVZ, Zambrano JRS. Diagnóstico y Características
Clínicas de la Tuberculosis Cutánea Asociada a Infección por VIH. Polo del Conocimiento: Revista
científico-profesional 2022;7(2):18.
7. Debrouwere I, Álvarez Vera PC, Pavón Benítez XDC, Rosero
Arboleda CK, Prinzie P, Lebeer J. Lessons from disability counting in ecuador, with a
contribution from primary health care. International Journal of Environmental Research and Public Health 2021;18(10):5103.
8. Correia MIG. Tuberculosis cutánea: revisión de la literatura. Dermatología Venezolana 2019;57(1).
9. World Health Organization. WHO consolidated guidelines on tuberculosis. Module 3: Diagnosis-Rapid
diagnostics for tuberculosis detection. World Health Organization. 2020.
10. Laxminarayan R. Economic
benefit of tuberculosis control. World Bank Publications 2007; 4295.