Sleep Apnea Revealing A Choanal Polyp Originating from the Middle Turbinate: A Case Report
INTRODUCTION
Choanal
polyps (CPs) are benign, solitary soft tissue lesions that extend to the
junction between the nasal cavity and the nasopharynx through the choana, and
sometimes extend into the oropharynx1. The most frequent
form is the antrochoanal polyp which originates from the maxillary sinus, but
there are other rarer localisation, such as polyps originating from the ostium
of the sphenoidal sinus, the inferior turbinate, the middle turbinate and the
inferior and middle meatus2-4. We report a rare case of
a patient who consulted for sleep apnea with right unilateral nasal obstruction
revealing choanal polyp originating from the middle turbinate that was removed
by an endoscopic surgery technique.
CASE REPORT
A 26-year-old male patient
presented with a 6months history of right nasal obstruction, sleep apnea, right
unilateral rhinorrhea and posterior discharge without epistaxis .He had no
significant past medical history. Endoscopic examination identified a big mass
in the lateral wall of the right choana, originating from the inferior portion
of the left middle concha, extending into the oropharynx and reaching the base
of the tongue. Examination of the oral cavity identified reddish-grey polypoid
mass filled the oropharynx (Figure 1).
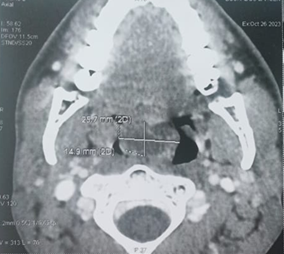
computed tomography (CT) scan of the of face revealed a mass of cystic density
filling the lumen of the nasopharynx and the upper part of the oropharynx which
was non-enhanced after contrast injection. However, all the paranasal sinuses
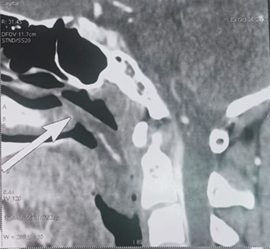
were clear (Figure 2). MRI of the
face revealed an oblong mass filling the lumen of the cavum originating in the
right nasal cavity opposite the middle meat and extending into the oropharynx (Figure 3). At surgery, the
nasopharyngeal part of the lesion and oropharyngeal part was debulked
endoscopically and transorally (Figure 4).
Histopathological analysis confirmed the diagnosis of Inflammatory sinonasal
polyp (Figure 5). 
Figure 1. Oropharyngeal
extension of nasal polyp.

(a) (b) (C)
Figure 2. Axial and sagittal sections of a CT scan of the face: shows a mass of cystic density which is inserted into the middle turbinate and extends into the nasopharynx (a,b) and oropharynx (a,b,c). 

(a) (b)
Figure 3. Coronal and
sagittal sections of a facial MRI: Insertion site of the mass in the middle
turbinate and extension into the nasopharynx (a) and oropharynx (b). 
Figure 4. The choanal polyp,
excised endoscopically and transorally.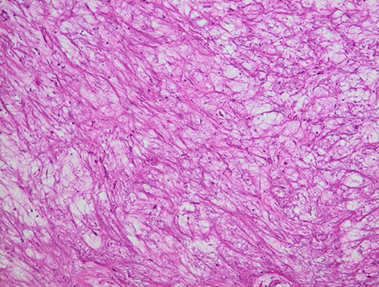
Figure 5. Histological section stained with hematoxylin and eosin (magnification
×20) the chorio is oedematous and the site of a polymorphic
inflammatory infiltrate composed of lymphocytes, plasma cells and neutrophils.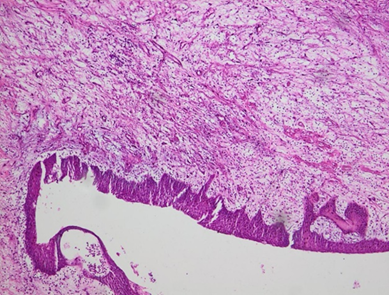
Figure 6. Histological
section stained with hematoxylin and eosin (magnification *20): The surface
coating is of respiratory type with squamous metaplasia.
DISCUSSION
The first description of
choanal polyps was reported by Killian5.
Based on what we currently understand, the maxillary or sphenoid sinus are
common sites where choanal polyps originate , particularly the antrochoanal
type, which constitutes approximately 6% of all nasal polyps choanal polyposis
typically affects a single sinus. There is compelling evidence indicating that
the antral or sphenoidal regions of choanal polyps consist of a cyst surrounded
by oedematous stroma6-8.Nevertheless,
in rare cases, they can originate from the anterior ethmoid, sphenoidal sinus,
nasal septum , inferior and middle turbinate8.
In 1906, Killian described the first case of a choanal polyp from the posterior
end of the middle turbinate9, and
only a few cases have so far been reported in the literature9-11.
Although varying in location,
CPs present in a similar manner and share similar symptoms and histological
findings. Nasal obstruction is the predominant symptom in a CP originating from
the middle turbinate10. Other
non-specific symptoms can be accompanied such as nasal congestion, hyposmia,
runny nose, mouth breathing and snoring if it extends into the oropharynx.
Epistaxis is not the usual revealing sign of a choanal polyp and should raise
suspicion of a nasopharyngeal fibroid in adolescents1.
One of the main
characteristics of CPs is the tendency for rapid growth, resulting in their
impressive dimensions. This
phenomenon may be attributed to heightened levels of basic fibroblast growth
factor (bFGF) and transforming growth factor beta (TGF-β) expression within CP tissue compared to
bilateral nasal polyposis and particularly healthy nasal mucosa12.
The differential diagnosis of
nasopharyngeal masses necessitates consideration of benign pathologies like
juvenile angiofibroma, teratoma, and meningoencephalocele, as well as malignant
conditions such as carcinoma, lymphoma, and sarcoma13-15.
Nasal endoscopic examination
and imaging techniques are commonly used to diagnose a CP and should be
considered before any definitive treatment. Imaging modalities such as computed
tomography paranasal sinus (CT) and magnetic resonance imaging are employed to
finding the attachment of the polyp, deciding the size of the polyp, and
diagnosis of concurrent sinusitis, all of which are crucial for therapeutic
effectiveness16. The choanal
polyp is hypodense on CT,
hypointense on T1-weighted and hyperintense on T2-weighted MR images, with peripheral
contrast enhancement. In cases involving vascular lesions, magnetic
resonance angiography of the nasopharynx may be indicated, there by rendering
it indispensable in the diagnostic process.
Surgery stands as the primary
recourse for treating CPs. Unlike nasal polyposis, steroid medications exhibit
minimal efficacy against CPs. Prior to the advent of endoscopic nasal surgery,
the Caldwell-Luc method and straight forward polyp removal were the predominant
surgical approaches for many years17.
Presently, endoscopic surgery emerges as the preferred treatment, offering a
favorable prognosis and minimal recurrence rates2,18,19.
Resection of CPs at their point of origin typically proves adequate, while for
antrochoanal polyps and sphenochoanal polyps, complete removal of the cystic
component within the maxillary and sphenoid sinuses is imperative to forestall
recurrence3,4,18,19.
CONCLUSION
In conclusion, it should be
kept in mind that CPs can originate from unusual locations. CT and MRI as well as nasal endoscopy
usually give precise definition of the polyp’s origin, thus preventing that
unaffected sinuses are operated on. Biopsy and histopathologic examination or
further imaging techniques (such as MRI) to avoid any missed diagnosis,
especially in instances with an atypical site of origin of CPs. The most
effective treatment is endoscopic removal of all cases of CPs.
REFERENCES
5. Killian G. The origin of choanal polypi. The Lancet
1906;4324: 81-82.
9. Prasad
U, Sagar PC, Shahul Hameed OA. Choanal polyp. J Laryngol Otol 1970;84(9):951‑954.