Solving the Diagnostic Challenge-Kidney Triplication with Ureterocele: The Indispensable Role of MR Urography
Abstract
Kidney triplication, also known as ureteral triplication, is
a rare congenital anomaly affecting the upper urinary tract. While the precise
embryological origin remains uncertain, it is thought to result from multiple
ureteric buds arising from the Wolffian duct during fetal development.
We present the case of a young girl with a triplex right
renal moiety with an associated ureterocele and Chiari malformation type 1. The
diagnosis was established through a comprehensive multi-modality imaging
approach, with MR Urography playing a pivotal role in solving the diagnostic
challenge. While ultrasound and scintigraphy provided initial insights, only
the high-resolution capability of MR Urography allowed for a definitive
characterization of the triplex collecting system, offering unparalleled clarity
that was essential for accurate diagnosis.
This case underscores the significance of advanced imaging
modalities in the diagnosis and management of such complex anomalies to guide
clinical decisions effectively.
Keywords: Kidney triplication; Ureteral triplication; MR
Urography
Background
Kidney triplication, also known as ureteral triplication, is
a rare congenital anomaly affecting the upper urinary tract. While the exact
embryological cause remains unclear, it is believed to arise from multiple
ureteric buds developing from the Wolffian duct during fetal development1,2.
This case report of a 6-year-old girl with right renal triplication &
ureterocele and Chiari malformation1, highlights the importance of a thorough
radiological workup for definitive diagnosis and guiding treatment decisions.
Clinical Presentation
The patient presented with a 2-year history of bed wetting
and recurrent UTIs, which prompted further investigation. A multi-modality
imaging approach was employed.
Ultrasound revealed a small sized right kidney with raised
parenchymal echogenicity and loss of cortico-medullary differentiation. The
right lower ureter was prominent and ended in an ureterocele.
Renal scintigraphy (EC scan) showed a marginally small right
kidney with optimal renal parenchymal function (40 %) and progressive excretion
pattern. The left kidney was normal.
Micturating cystourethrogram (MCU) was normal and there was
no vesico-ureteric reflux.
MR Urography confirmed a small right kidney with triplex
collecting system, with ectopic opening of the right upper moiety ureter at the
neck of the urinary bladder. The two lower moiety ureters on the right showed
fusion of their draining ureters at the L4 vertebral level, draining into the
right vesico-ureteric junction.
MR Brain and spine screening revealed peg-like tonsillar
herniation with formation of a syrinx in the cervical cord was seen indicative
of Chiari Type I malformation.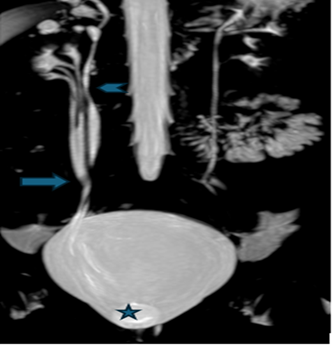
Figure 1: MR Urography coronal MIP Image
shows right kidney with triplex collecting system, The lower two moieties on
the right show fusion of the ureters at the L4 vertebral level ( ) draining normally into the right
vesico-ureteric junction, terminating into a ureterocele (
) draining normally into the right
vesico-ureteric junction, terminating into a ureterocele (  ). The upper moiety ureter is marked by
). The upper moiety ureter is marked by 
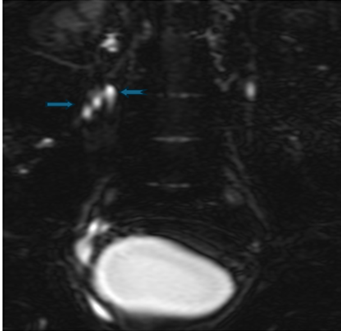
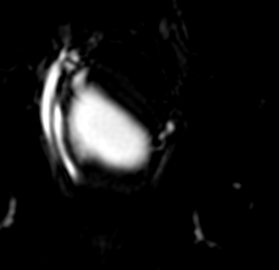
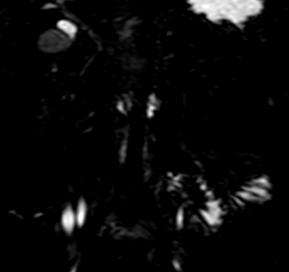
Figure 2 (a,b,c): MR Urography image
shows the two laterally placed right lower ureters, fuse at the level of L4
vertebral body (  ) and terminate into
the vesico-ureteric junction; whereas the single upper moiety ureter terminates
ectopically into the neck of the bladder (
) and terminate into
the vesico-ureteric junction; whereas the single upper moiety ureter terminates
ectopically into the neck of the bladder (  )
)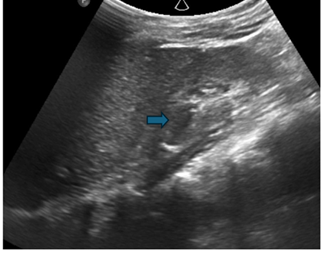
Figure 3: Ultrasound image of the right
kidney showing a triplex collecting system (  ) with focal upper moiety
caliectasis. An increased parenchymal echogenicity and loss of
cortico-medullary differentiation
) with focal upper moiety
caliectasis. An increased parenchymal echogenicity and loss of
cortico-medullary differentiation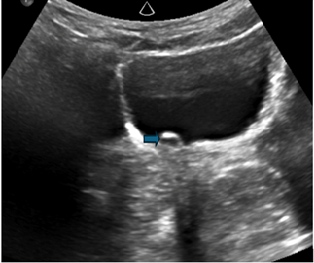
![]()
Figure 4: Ultrasound image of the
urinary bladder reveals a prominent right ureter terminating in a ureterocele (  )
)
Discussion
Classification
Smith's classification system categorizes ureteral triplication into four types based on the number of ureters and ureteral orifices3. Our case falls under type 2, with three ureters and two ureteral orifices (incomplete triplication).
|
Type |
Smith Classification
|
|
A |
Triple ureters, (Complete triplication) Three separate ureters and
three separate ureteral orifices in bladder, urethra or ectopic location.
(35%)
|
|
B |
Incomplete triplication Three ureters arise from the kidney. Two joins
on the way to the bladder and two orifices present in the bladder (21%)
|
|
C |
Trifid ureter. All three ureters unite and drain through a single
orifice (31%)
|
|
D |
Two ureters from the kidney. One divides into two to have three
draining orifices (9%) |
Importance
of imaging in diagnosis
A
precise diagnosis of urinary tract anomalies requires a multimodality imaging
approach, with each technique providing distinct structural and functional
insights.
Ultrasound
is the first-line imaging tool due to its easy accessibility and non-invasive
nature, identifying obvious anatomical abnormalities such as duplex moieties,
dilated ureters with duplication and ureteroceles. Intravenous urography (IVU),
has been particularly useful in detecting anomalies like Smith’s type two
ureteral triplication. Micturating cystourethrogram (MCU) plays a key role in
evaluating the lower urinary tract and diagnosing vesico-ureteric reflux (VUR),
a frequent complication of ureteral anomalies. Renal scintigraphy provides
functional assessment of the kidneys, helping to identify impairments in the
collecting system and overall renal function1.
MRU
emerges as the gold standard for detailed anatomical and functional evaluation
of the urinary system, offering superior and unparalleled visualization of
complex urinary tract anomalies. MRI, due to its non-ionising nature, has
proven valuable in detecting concurrent embryological and developmental
conditions, particularly in the pediatric age group; highlighting its
indispensable role in a comprehensive diagnostic workup1,4. However, it does require patient
cooperation and sometimes sedation in pediatric patients to minimize movement
during the scan2,6.
Discussion
Understanding
the clinical significance of ureteral triplication is vital for proper
management. While incontinence, recurrent urinary tract infections (UTIs) and
abdominal pain are prominent presenting signs, the illness often manifests
asymptomatically. In some cases, patients may develop complications such as
obstruction, reflux and renal dysfunction, which necessitate prompt and
appropriate intervention1,6.
Management
strategies for ureteral triplication depend on the severity of symptoms, the
presence of complications and the overall functional status of the kidneys.
Observation may be sufficient for asymptomatic patients, while those with
recurrent UTIs require appropriate antibiotic management to prevent
complications. Minimally invasive laparoscopic techniques are indicated for
patients with ongoing obstruction or deteriorating renal function1,2,4.
This
6-year-old girl with right renal triplication and a ureterocele is a complex
and rare congenital anomaly which requires expeditious diagnosis. The
integration of various imaging modalities, as demonstrated in this report,
aligns with the findings of previous studies, highlighting the evolution of
diagnostic techniques over time.
Ureteral
duplication is the primary differential for triplication, as both anomalies
involve multiple ureters draining a single kidney and share complications like
reflux, obstruction and ureteroceles. However, distinguishing between them is
critical for management. Ultrasound and IVU have limitations, often failing to
detect an additional ureter due to poor resolution or contrast filling issues.
MRU is the gold standard, offering high-resolution, multiplanar visualization,
superior tissue contrast and functional assessment. MRU allows accurate
differentiation between duplication and triplication, facilitating optimal
treatment planning1,6.
Another important differential diagnosis is
renal dysplasia, a condition characterized by abnormal kidney development,
leading to cyst formation and impaired renal function. Where modalities like
USG and IVU fail, MRU plays a crucial role in differentiating renal dysplasia
from triplication by identifying structural abnormalities and assessing the
presence of multiple collecting systems1,2.
Ureteral
triplication often occurs alongside other congenital anomalies, further
complicating their diagnosis and management. Contralateral duplication is the
most frequently associated anomaly, reported in 37% of cases2. Additionally, ureteral ectopia is
observed in 28% of cases, while renal dysplasia is noted in 8%5. Another significant concern is
vesicoureteral reflux (VUR), which can arise as a consequence of obstruction,
particularly in the presence of a ureterocele2.
Recognizing these coexisting anomalies is essential for comprehensive
evaluation, as they influence both clinical presentation and treatment
strategies.
Conclusion
The
discussion emphasizes how crucial it is to use a multidisciplinary approach
when diagnosing and treating ureteral triplication, involving radiologists,
urologists and pediatric surgeons. Using sophisticated imaging methods such as
MRU, can provide comprehensive anatomical and functional data that is critical
for informing therapy choices, thereby allowing medical practitioners to
proficiently handle this uncommon condition and improving the well-being of
those impacted.
2. Solomon IP, Klein I, Dekel Y. Urosepsis and abscess in an adult with a triplicated renal collecting system treated percutaneously and endoscopically. Radiol Case Rep 2021;17(2):275-278.
3. Osipov IB, Lebedev DA, Lifanova MV. Kidney triplication with ectopic ureterocele: a case report. BMC Urol 2020;20:54.
4. Singh TR, Dhua AK, Agarwala S, Yadav R, Kandasamy D, Kumar R. Triplication of Ureter: A Rare Case. J Indian Assoc Pediatr Surg 2022;27(1):91-93.
5. Al-Zubi M, Al Faqieh A, Altamimi O, Albeitawi S. Unilateral triplicate ureter with ipsilateral ureterocele a case report. Int J Surg Case Rep 2020;70:178-181.
6. Mubarak MY, Zainun AR, Rohaya M. Ureter triplication with contra-lateral partial duplex system. Med J Malaysia 2009;64(3):236-237.