Survival Against the Odds: An Exceedingly Uncommon Case of Type A3 Truncus Arteriosus in an Adult Male Thriving without Surgical Intervention
Abstract
Persistent truncus arteriosus is an uncommon complex congenital heart disease. Without surgical intervention, the prognosis is not good. Very few untreated cases of truncus arteriosus survive to maturity. We report an exceptional case of uncorrected truncus arteriosus surviving into adulthood of type a3 variant -van praagh classification as a 26-year-old male who had well tolerated dyspnea since birth. Our patient showed a single(right) pulmonary artery arising from the common arterial trunk supplying the right lung and absent main and left pulmonary artery with collateral supply to the left lung consistent with the truncus arteriosus type a3-van praagh classification
Keywords: persistent truncus arteriosus; congenital heart disease; surgical intervention; van praagh; arterial trunk
Introduction
Truncus arteriosus usually presents early after birth and accounts for 1% of congenital heart disease1. It is typified by the truncus arteriosus failing to split during fetal development into the pulmonary and aortic arteries, resulting in a single artery with different properties. Among the four subtypes of truncus arteriosus, type iv has a relatively longer survival rate due to low pulmonary blood flow, while types i, ii and iii have significantly worse outcomes, with 80% of infants dying before reaching infancy. This is because of the increased incidence of heart failure due to higher pulmonary blood flow, which causes mortality2.
Since the prognosis for types 1 - 3 is so bad, very little is known about their natural, unrepaired course. However, there have been very few cases of survivorship beyond infancy without intervention3. Echocardiography might not always be helpful in assessing this kind of chd. Recognition of this chd is facilitated by its presence on computed tomography (ct). We talked about the ct imaging features of case of type a3 truncus arteriosus in our case report.
Case presentation
A 25-year-old male presented to cardiology opd at jawaharlal nehru medical college, a tertiary care hospital, with complaints of well-tolerated breathlessness since childhood. He weighed 40 kilograms and stood 156 cm tall. Evidence of clubbing with no cyanosis. His blood pressure was 128/64 mmhg and his heart rate was 88/min. The spo2 measurement using pulse oximetry was 98% and pansystolic murmur on auscultation was recorded. Echocardiography revealed a single common arterial trunk, large mal-aligned vsd with mild ar and a diagnosis of hemi-truncus was made4.
A multi-phasic cardiac ct demonstrated cardiomegaly with a single common arterial trunk or truncus arteriosus (figure 1) and an only pulmonary artery emerging from the postero-lateral aspect of common arterial trunk above the valvular level was noted to have tortuous course and ultimately supplying the right hilum i.e. Right pulmonary artery (figures 2a& 2b). Main pulmonary artery and pulmonary artery for left hilum were absent. Two mapcas (major aortopulmonary collateral arteries) supplied the right lung (figures 3,4), while the left lung was supplied by few minor collaterals (figures 5,6). An associated large membranous ventricular septal defect was noted (figures 7,8).
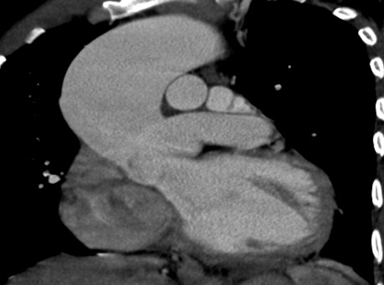
Figure 1: coronal ct scan shows a common arterial trunk arising from left ventricle with over-riding of aorta and vsd

Figure 2a axial ct: a pulmonary artery arising from the posterolateral aspect of common arterial trunk (truncus) from its posterolateral aspect and continuing as right pulmonary artery supplying right hilum

Figure 2b 1 axial ct: a pulmonary artery arising from the posterolateral aspect of common arterial trunk (truncus) from its posterolateral aspect and continuing as right pulmonary artery supplying right hilum

Figure 3axial ct: a pulmonary artery arising from the posterolateral aspect of common arterial trunk (truncus) from its posterolateral aspect and continuing as right pulmonary artery supplying right hilum

Figure 4axial ct: a pulmonary artery arising from the posterolateral aspect of common arterial trunk (truncus) from its posterolateral aspect and continuing as right pulmonary artery supplying right hilum

Figure 5axial ct: a pulmonary artery arising from the posterolateral aspect of common arterial trunk (truncus) from its posterolateral aspect and continuing as right pulmonary artery supplying right hilum
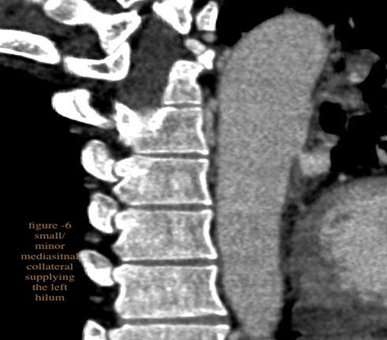
Figure 6axial ct: a pulmonary artery arising from the posterolateral aspect of common arterial trunk (truncus) from its posterolateral aspect and continuing as right pulmonary artery supplying right hilum
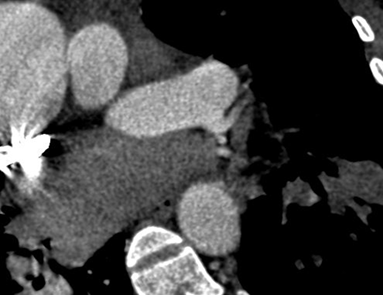
Figure 7axial ct: a pulmonary artery arising from the posterolateral aspect of common arterial trunk (truncus) from its posterolateral aspect and continuing as right pulmonary artery supplying right hilum

Figure 8axial ct: a pulmonary artery arising from the posterolateral aspect of common arterial trunk (truncus) from its posterolateral aspect and continuing as right pulmonary artery supplying right hilum
The left major coronary artery exhibits an abnormal origin from the proximal aspect of the right pulmonary artery, which further divided into left anterior descending artery and left circumflex artery (figures 7 and 8). Right coronary artery has got its origin directly from common truncus.
Associated pulmonary artery hypertension with mosaic attenuation in bilateral lung fields were reported (figure 5). Right heart strain was indicated by a contrast-related reflux from the right atrium into the inferior vena cava and hepatic veins.
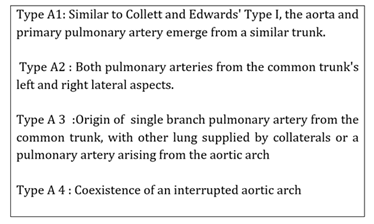
Our patient showed truncus arteriosus with only rpa supplying right lung and absent mpa and lpa. A final diagnosis of type a3 truncus arteriosus (van praagh classification) was made. It is defined when single pulmonary artery that originates from the common trunk supplying one lung, while the other lung is fed by collateral arteries or a pulmonary artery emerging from the aortic arch5. {video uploaded &vrt images-1& 2}
The modalities of the treatment, including the need for cardiac transplantation, were discussed with the family. However, the patient denied surgery and has been on regular follow-up for 1 year and has shown no worsening of symptoms.
Discussion
Persistent truncus arteriosus is a rare cyanotic congenital heart disease which is defined when single arterial trunk arises form the ventricle and is accompanied by large ventricular septal defect. While constituting fewer than 1% of the total number of congenital heart defects, the annual incidence is 7 per 100,000 live births and constitutes for 4% of severe congenital heart diseases6.
The two main classification schemes for the truncus arteriosus are the van praagh & van praagh classification (1965) and the collett and edwards classification (1949).
Collett and edwards classification7
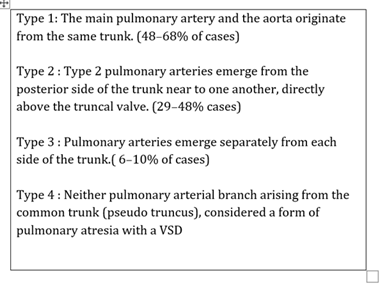
Van praagh modified classification5
In younger age groups, surgical surgery entails total correction through vsd closure and pulmonary artery to right ventricle connection2. Patients who have acquired pulmonary hypertension may undergo shunt procedure as palliative approach or dilation, may or may not involve the mapca stenting. Although there may be some benefit, the utility of medical management using phosphodiesterase-type 5 inhibitor sildenafil and endothelin antagonist is still not clear8.
In our case, truncus arteriosus with single pulmonary artery (large aorta type with the absence of other pulmonary artery) falls under type a3 variant. Desaturated blood is expelled into the single outflow tract due to mixing of pulmonary circulation blood and systemic circulation at vsd level. Major aortopulmonary collaterals offer high pressure pulmonary flow, which contributes to pulmonary arterial hypertension since the right pulmonary arteries directly arise from the truncus arteriosus. Heart failure is brought on by increased burden on the heart and lungs due to altered perfusion and ventilation mismatches. Larger mapcas and non-obstructive pulmonary arteries were the natural phenomenon for masking patient symptoms. Associated anomalous coronary artery and pah have rendered this patient inoperative.
Embryologically, these lesions result from anomalies in the left sixth arch and cono-truncal anomalies. Digeorge syndrome is typically linked to it9; however, a genetic investigation of our case has been planned.
After reviewing the literature, to the best of our knowledge, truncus arteriosus with this kind of modified van praagh's type 3a surviving up to 26 years of age without need for surgery has not been documented in the literature till date. The survival of our patient offers information on the natural progression of the uncommonly complex congenital heart disease. The oldest similar reported case of this type of truncus was a 12-year-old child who survived without surgery10.
Conclusion
Our case, the patient with type a3 variant has survived till 26 years of age without any surgical intervention which makes it worthy of reporting.
Our case is one of the rare cases where a man of this variant of truncus has made it into his 3rd decade without surgery.
References
1. hoffman jie, kaplan s. The incidence
of congenital heart disease. J am coll cardiol 2002;39(12):1890-900.
2. Baggen vjm, connelly
ms, roos-hesselink jw. Truncus arteriosus. In: diagnosis and management of
adult congenital heart disease 2018;421-428.
3. choudhary v,
biradar s, hirapur i, chanda s. A rare case of truncus arteriosus in the
elderly. Apik j intern med 2019;7:131.
4. talwar s,
meena a, ramakrishnan s, choudhary sk, airan b. Hemitruncus with ventricular
septal defect in a 6-year-old child. Ann pediatric cardio 2013;6(2):194-196.
5. van praagh r, van praagh s. The
anatomy of common aorticopulmonary trunk (truncus arteriosus communis) and its
embryologic implications. Am j cardiol 1965;16:406-425.
6. liu y, chen s, zühlke l, black gc,
choy m kit, li n, et al. Global birth prevalence of congenital heart defects
1970-2017: updated systematic review and meta-analysis of 260 studies. Int j
epidemiol 2019;48:455-1463.
7. collett rw, edwards je. Persistent
truncus arteriosus: a classification according to anatomic types. Surg clin
north am 1949;29(4):1245-1270.
8. dimopoulos k, diller gp, opotowsky
ar, d’alto m, gu h, giannakoulas g, et al. Definition and management of
segmental pulmonary hypertension. J am heart assoc 2018;7(14):008587.
9. Abhilash t, satheesan
p, kumar r. Clinical management of congenital heart disease from infancy to
adulthood. Ann pediatr cardiol 2015;8(1):93.
10. vijayakumar
v, muthuramalingam s, ganesamoorthi a. Truncus arteriosus - modified van
praagh’s type 3a and anesthesia: a case report. Ain-shams j anesthesiol
2020;12:11.
11. calder l, praagh rv, praagh sv, et
al. Clinical, angiocardiographic and pathologic findings in 100 patients. Am
heart j 1976;92(1):23-38.
12. abid d,
daoud e, koubaa s, et al. Unrepaired persistent truncus arteriosus in a
38-year-old woman with an uneventful pregnancy. Cardiovasc j afr 2015;26:68.