Transverse Myelitis in a Middle-Aged Patient: A Case Report
Abstract
Transverse myelitis (tm) is a rare inflammatory disease affecting the spinal cord, leading to motor, sensory, and autonomic dysfunctions. This condition can be idiopathic or secondary to various etiologies, including infections, autoimmune diseases, and post-infectious events. Clinically, tm is characterized by the rapid onset of bilateral symptoms, potentially progressing to paraplegia or tetraplegia with varying severity. Studies have indicated a connection between transverse myelitis and demyelinating diseases such as multiple sclerosis and neuromyelitis optica.
Key words: spinal
cord; inflammation; magnetic resonance imaging; neuroimmunology
Introduction
Transverse myelitis (tm) is a rare
neurological condition characterized by spinal cord inflammation, causing
diverse neurological deficits that affect motor function, sensation, and
autonomic processes. The term "transverse" refers to inflammation
spanning the spinal cords width, often leading to bilateral symptoms1. Tm is classified as a rare neuroimmunological
disease, presenting abruptly and, in some cases, progressively, with
symmetrical or asymmetrical signs and symptoms along the spinal cord. The
causes of this disease can be idiopathic, associated with autoimmune disorders,
viral infections or even complications from medical conditions like multiple
sclerosis and systemic lupus erythematosus. Its diverse etiology includes
infectious processes, autoimmune diseases, and reactions to biological agents
such as vaccines2-5. Among the
best-known autoimmune causes are multiple sclerosis (ms) and neuromyelitis
optica (nmo), conditions with similar clinical presentations, complicating
differential diagnoses. Early diagnosis and management of transverse myelitis
are essential to minimize neurological sequelae. Clinical manifestations can
range from mild motor deficits to complete paralysis and sensory loss below the
lesion level. Complementary exams, such as magnetic resonance imaging (mri) and
cerebrospinal fluid analysis, are crucial for differential diagnoses6.
Objective
This study aims to describe a clinical case of a young patient and
discuss the main causes, differential diagnoses, treatment options, and
prognosis of transverse myelitis.
Materials and methods
A retrospective case report was prepared through electronic medical
record research and supported by a brief literature review using the pubmed and
scielo databases.
Case report
A 36-year-old male patient was admitted to the
hospital with complaints of paresis associated with myalgia and action tremor,
ascending and symmetrical in nature, with onset 7 days prior. For the past 3
days, he has been unable to walk without assistance. He also reported
difficulty sustaining upper limbs and feeding himself, with no other
complaints. The patient mentioned having had flu-like symptoms about 20 days
before admission and was on the 5th postoperative day of laparoscopic
cholecystectomy for biliary pancreatitis. However, as noted, the current
symptoms started before the surgery, raising the diagnostic hypothesis of
guillain-barré syndrome. Laboratory
tests, including electrolyte screening and cranial ct, showed no abnormalities.
Several differential diagnosis tests were performed, including lumbar puncture,
which revealed no cerebrospinal fluid (csf) cell-protein dissociation, ruling
out meningitis. Serologies for syphilis, hepatitis a, hepatitis b, and hiv were
all non-reactive. During hospitalization, the patient remained hemodynamically
stable without respiratory complaints, walking with assistance and undergoing
physiotherapy. He maintained grade 1 paresis in the lower limbs and grade 3 in
the upper limbs. Lumbar ct showed a slight l4-l5 intervertebral disc bulge, and
cervical ct revealed subcortical sclerosis and small marginal osteophytes in
the odontoid process and anterior arch of the atlas. A neurologist recommended
icu admission due to the possibility of respiratory failure and prescribed
immunoglobulin at 2g/kg over 5 days. Upon icu admission, neurological
examination showed altered strength in all four limbs, grade 2 paresis in the
lower limbs, and grade 3 in the upper limbs, with preserved neck mobility and
no aphasia. After returning to the ward, the patient experienced worsening
weakness in both upper and lower limbs, becoming unable to walk and presenting
reduced reflexes, swallowing difficulty for solids, but no visual acuity
impairment. A new csf analysis showed no abnormalities. Neurological evaluation
led to icu readmission and a second cycle of immunoglobulin at 2g/kg for 5
days. Cervical spine mri showed small posteromedian disc protrusions at c5-c6
and c6-c7 without spinal cord compression. Brain mri revealed a residual hemosiderin
focus in the left frontal periventricular white matter. Thoracic spine mri
showed mild signal alteration in the central thoracic medullary segments,
raising the possibility of transverse myelitis. Following these findings,
corticosteroid pulse therapy (methylprednisolone 1g/day for 5 days) was
initiated in consultation with neurology. Despite these measures, the patient
showed no significant improvement. After 10 days in the icu, he was transferred
back to the ward for rehabilitation and continued investigations. Throughout
hospitalization, the patient underwent various medication protocols and
received multidisciplinary care, including physiotherapy and speech therapy.
Given the limited treatment response, transfer to a tertiary care center with
greater technological support was arranged for possible plasmapheresis (figure
1).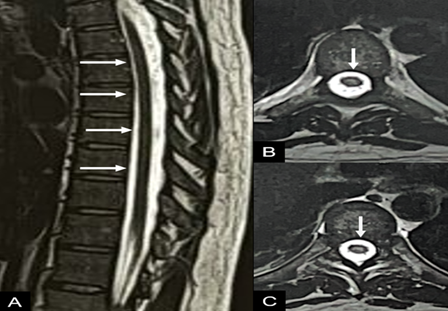
Figure 1: sagittal (a) and
axial (b) t2-weighted images of the thoracic spine, showing a slight area of
signal alteration in the central portion of the spinal cord (arrows in a and
b).
Discussion
Transverse myelitis presents a broad range of clinical
manifestations that vary according to the extent and location of spinal cord
inflammation. Major symptoms include back pain, flaccid or spastic paralysis,
sphincter dysfunction, and sensory deficits, often appearing rapidly7-9. The variability in symptom severity
reflects the condition's etiological heterogeneity, involving infectious,
autoimmune, and even traumatic factors.
The diagnosis is typically based on clinical examination and confirmed
through imaging studies, such as mri, and laboratory tests, including
cerebrospinal fluid analysis10. Mri
often reveals inflammation, while cerebrospinal fluid analysis frequently shows
lymphocytic pleocytosis and elevated protein levels, aiding in distinguishing
tm from other neurological conditions like infections and spinal neoplasms. Treatment
options include high-dose corticosteroids, intravenous immunoglobulin, and
plasmapheresis in certain cases11.
Therapeutic approaches vary based on the suspected etiology, with early
intervention being most effective. In refractory or recurrent cases,
immunomodulatory therapies such as rituximab have been explored. Prognosis
remains uncertain, with recovery often being partial and dependent on the
initial severity and timeliness of treatment initiation. Studies suggest that
approximately one-third of patients recover fully, one-third experience mild to
moderate sequelae, and another third sustain significant deficits12.
Conclusion
Transverse myelitis poses a clinical challenge
due to its etiological variability and unpredictable treatment response. Early
recognition and proper management are crucial to improving prognosis and
reducing long-term complications. Advances in imaging techniques and
immunomodulatory treatments hold promise for substantial improvements in
managing this condition. Recent developments in neuroimaging and laboratory
testing, such as aquaporin-4 (aqp4-igg) and myelin oligodendrocyte glycoprotein
(mog) antibody assays, have enabled better differentiation of tm from other
demyelinating diseases, particularly neuromyelitis optica. Despite the
limitations of current treatments, progress in understanding tm pathophysiology
may pave the way for more effective and targeted therapies. Although existing
treatments show benefits in reducing inflammation, there is a growing need for
more focused therapeutic strategies.
Ethical statement
Informed
consent has been provided by the patient for publication of this case report.
References
1. krishnan c, kaplin ai, pardo ca, kerr da, keswani sc. Demyelinating
disorders: update on transverse myelitis. Current neurology and neuroscience
reports 2006;6(3):236-243.
2. bhat
a, naguwa s, cheema g, gershwin me. The epidemiology of transverse myelitis.
Autoimmunity reviews 2010;9(5):395-399.
3. pidcock
fs, krishnan c, crawford to, salorio cf, trovato m, kerr da. Acute transverse
myelitis in childhood: center-based analysis of 47 cases. Neurology 2007;68(18):1474-1480.
4. greenberg
bm, thomas kp, krishnan c, kaplin ai, kerr da. Idiopathic transverse myelitis:
corticosteroids, plasma exchange or cyclophosphamide. Neurology 2007;68(21):1614-1617.
5. beh
sc, greenberg bm, frohman t. Transverse myelitis. Neurologic clinics 2013;31(3):557-583.
6. transverse
myelitis consortium working group. Proposed diagnostic criteria and nosology of
acute transverse myelitis. Neurology 2002;59(4):499-505.
7. scott
tf, frohman em, de seze j, gronseth gs, weinshenker bg. Evidence-based
guideline: treatment of paralyzing acute transverse myelitis in adults. Report
of the therapeutics and technology assessment subcommittee of the american academy
of neurology. Neurology 2011;77(20):2124-2130.
8. berman
m, feldman s, alter m, zilber n, kahana e, miller a. Acute transverse myelitis
incidence and etiologic considerations. Neurology 1981;31(8):966-971.
9. kerr
da, ayetey h. Immunopathogenesis of acute transverse myelitis. Current opinion
in neurology 2002;15(3):339-347.
10. jeffery
dr, mandler rn, davis le. Transverse myelitis: retrospective analysis of 33
cases, with differentiation of cases associated with multiple sclerosis and parainfectious
events. Arch neurol 1993.
11. kaplin
ai, krishnan c, deshpande dm, et al. Diagnosis and management of acute
myelopathies. Neurologic clinics 2004;22(2):389-405.
12. west
tw. Transverse myelitis-a review of the presentation, diagnosis, and initial
management. Discovery med 2013;16(88):167-177.