Twenty-Year-Old Female with Takayasu Arteritis and Pulmonary Tuberculosis: A Case Report
Keywords: takayasu arteritis; tuberculosis; vasculitis
1.
Introduction
Takayasu arteritis is a chronic granulomatous vasculitis of large vessels that affects the aorta and its main branches. This granulomatous inflammation may lead to stenosis, occlusion, dilatation, or aneurysm of the involved arteries1. Although takayasu arteritis is frequently seen in young women, it can also affect young infants and adolescents2. Takayasu arteritis in childhood is rare, with only 2.6/1 000 000 of childhood-onset takayasu arteritis reported in literature until now3. Features are variable depending on the stage of disease. In fact, the first stage of initial inflammatory process is often unrecognized and characterized by systemic signs4. In the second stage, multiple arterial occlusions. And stenosis can occur, and can be revealed by signs of cerebral, visceral, or extremity ischemia4.
Takayasu arteritis also known as “pulseless disease," is an uncommon, chronic granulomatous vasculitis that mainly affects the large arteries such as the aorta and its primary branches5. It was initially described in 1908 by dr. Mikito takayasu, a professor of ophthalmology at kanazawa university, japan6. One in 200,000 person is affected by takayasu arteritis, it predominantly affects females under 40 years with a female to male ratio of 9:15,6. Takayasu arteritis occurs in every part of the world; however, it is more common in southeast asia, india, japan, china, korea, mexico, and latin america5,4.
Takayasu arteritis can be present in two phases, a systematic phase followed by an occlusive phase6. The first phase shows non-specific constitutional symptoms such as fever, myalgia, fatigue, anorexia, weight loss, tenderness in the affected arteries6,4. The acute phase reactant such as erythrocyte sedimentation and c reactive protein is usually raised in this phase6,7. The second phase occurs due to chronic inflammation and stenosis of the involved arteries, resulting in claudication of the limb, headache, dizziness, hypertension, chest pain, blood pressure discrepancies between two arms, and diminished or absent peripheral pulses5,8. It is characterized by the infiltration of inflammatory cells in tunica media, hyperplasia of the intima, and thickening of adventitia, histologically9.
Tuberculosis is a curable and treatable disease that is distributed worldwide10. According to world health organization (who), in 2019, the most significant number of tuberculosis cases was seen in the who southeast asian region11. Tuberculosis affects all age groups, adults being the most commonly affected population10. It is a transmissible bacterial infection caused by mycobacterium tuberculosis, it is transmitted via the respiratory route and iti chiefly affects the lungs12. Nonetheless, other tissues and organs may also be involved11. Although one-fourth of the world's population is infected with tuberculosis, most of them only have latent tuberculosis within their lifetime; the rest of the affected individuals effectively contain their infection11. The risk of reactivation of latent to active tuberculosis is most significant in people with immune-deficient conditions12.
The precise etiology of takayasu arteritis continues to be unknown5. However, autoimmunity is mainly suggested as a cause of takayasu arteritis13. The other causes that might contribute to takayasu arteritis's etiopathogenesis are genetic and infectious (bacterial, viral) causes6,13. Of the bacterial causes, the role of mycobacterium tuberculosis has been implied14. Takayasu arteritis is one of the first vasculitides to be related to a particular infective organism14. Initially, this likely co-relation was mentioned due to the morphological resemblance of langhan’s giant-cell granulomas with tuberculous lesions15. Another likely finding signifying this correlation is the evidence of tubercular lymph nodes in the arterial lesions, increased agalactosyl igg level, augmented responses to purified protein derivative of mycobacterium tuberculosis13,16,17. In addition, recent studies suggest the role of mycobacterial heat shock protein (hsp) in linking autoimmune disease and mycobacterium tuberculosis18. The molecular cross-reactivity between host hsps and mycobacterial hsps could be the probable trigger for the autoimmune process18. Also, in takayasu arteritis patients' aortic tissues, soto et al. Detected an increased frequency of is6110 and hupb genes19. Takayasu arteritis is commonly seen in east asia or southeast asia, where the prevalence of tuberculosis is high20.
In this case report aimed to examine and consolidate the relevant information on this connection. And, it intends to highlight the association between mycobacterium tuberculosis and takayasu’s arteritis and the possible cause for this link from the studies done previously.
2. Case presentation
A
20-year-old woman presented with abdominal and neck pain. Her medical history
was unremarkable. Physical examination showed pulseless left brachial and
radial arteries, decreased right brachial and radial artery pulses. There was a
blood pressure difference between arms (right arm: 101/59 mmhg; left arm 90/51
mmhg). The presence of bruits over left subclavian and left common carotid
artery. High sensivity crp was elevated 206.7 mg/l (≤ 3 mg/l), erythrocyte
sedimentation rate was elevated 124 mm (first hour) and 136 mm (second hour).
Ana test was negative, anti dsdna was negative, anca screen was negative, tsh,
free t4 was normal, mild hypochromic microcytic anemia with hb:
10 g/dl, high white blood cell with 14.63 x109/l, platelet 593 x 109/l.
Electrocardiography showed sinus tachycardia 120 bpm (figure 1). Chest x-ray showed normal findings (figure 2). Carotid ultrasound revealed concentric thickening of the
left common carotid artery with 70% stenosis. Chest and abdomen aortic ct scan
with contrast showed stenosis of the right brachiocephalic artery, left common
carotid artery, 50% stenosis of the left subclavian artery and 60% stenosis of
the right renal artery (figure 3).
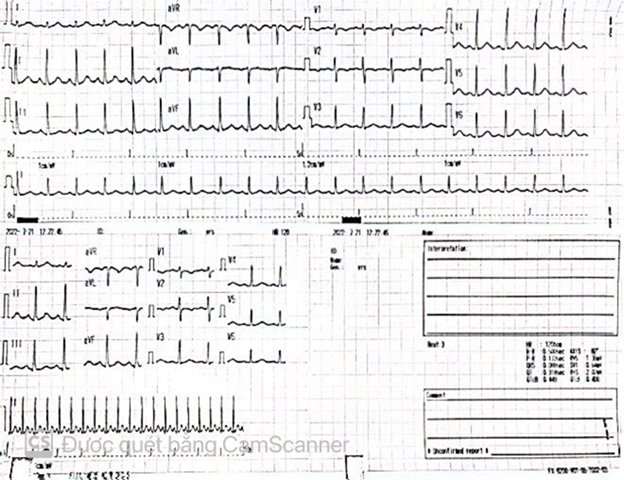
Figure 1. Electrocardiography showed sinus
tachycardia 120 bpm.
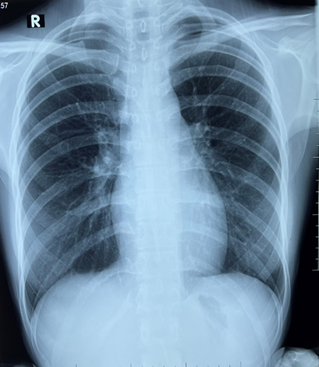
Figure 2. Chest x-ray appears unremarkable
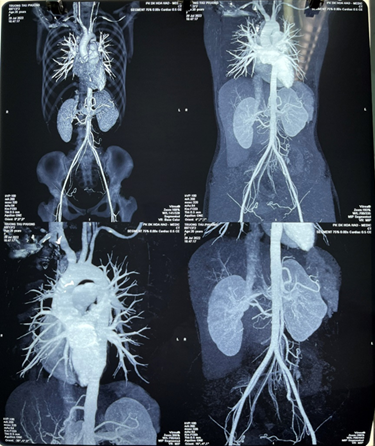
Figure 3. Chest and abdomen aortic ct scan with
contrast showed stenosis of the right brachiocephalic artery, left common
carotid artery, 50% stenosis of the left subclavian artery and 60% stenosis of
the right renal artery.
After
physical and systemic examination, we suspect that this patient has takayasu
arteritis because of having 4 over 6 criteria: onset age ≤ 40 years; decreased
brachial artery pulse; > 10mmhg difference in systolic blood pressure
between arms; a bruit over subclavian or aorta arteries according to the
american college of rheumatology 1990 criteria21
for the classification of takayasu arteritis with a sensitivity of 90.5% and a
specificity of 97.8%. The chest and abdominal ct angiography showed moderate
renal artery stenosis (60%). 50% stenosis of the left common carotid artery.
Patient was prescribed prednisone 1mg/kg daily. Unfortunately, after taking
corticosteroids, the patient coughed a lot and had a fever in the afternoon.
The patient had a chest x-ray with suspicion of pulmonary tuberculosis. The
patient was tested for xpert gene; the result was positive. The patient was
treated with a 9-month anti-tuberculosis regimen rifampicin, isoniazid,
pyrazinamide, and ethambutol with prednisone 5mg/day. The patient continued
taking prednisone for 2 years. Follow-up was favorable clinically, biologically,
and radiologically.
1. Discussion
In
2017, zhang et al. Reported an unusual case of pulmonary tuberculosis diagnosed
six months after takayasu arteritis was diagnosed22.
Clemente et al. Conducted a retrospective observational study to describe
takayasu arteritis clinical and angiographic features in 71 brazilian children
and adolescents23. Their research
revealed a higher frequency of tuberculin skin test positivity in their
patients than healthy brazilian children, as reported by the brazilian
institute of geography and statistics23.
This finding hints at the prevalence of latent tuberculosis in a patient with
takayasu arteritis. Although the exact etiology could not be identified,
clemente et al. Highlighted that the immune response in takayasu arteritis
could be a result of cross-reaction between homologous protein present in the
vascular wall of the host and the mycobacterial heat shock 65-kd23.
Similarly,
a cross-sectional study conducted by nooshin et al. Found the level of
purified-protein derivative >10mm in six out of 15 study subjects, stressing
the association of latent tuberculosis in a patient with takayasu arteritis25.
Furthermore, in 2010, al-aghbari et al. Demonstrated a particular case of
takayasu arteritis who had a strongly positive mantoux test for tb18. This was the first-ever case of takayasu
arteritis associated with tuberculosis in yemen19.
Lastly, the findings of muranjan et al. Highlighted the correlation between
infection with mycobacteria tuberculosis and takayasu arteritis pathogenesis,
who detected positive tuberculin skin test or bacille calmette-guerin (bcg) in
six (35.2%) out of 17 patients with takayasu arteritis25-27.
Although
there is no evidence that anti-tuberculosis therapy prevents takayasu arteritis
progression or its complications, the combination of corticosteroids and anti-
tuberculosis drugs was efficient to control the disease activity observed in
our patient.
2. Conclusion
We
conclude that takayasu arteritis must be suspected when there were blood
pressure differences between extremities. A causal relationship between
tuberculosis and takayasu arteritis and evidence of prevention of takayasu
arteritis progression and complications under anti-tuberculosis therapy need
further investigation. In takayasu arteritis, a close monitoring of the
clinical disease activity and damage associated with inflammatory markers and
imaging are necessary to better identify the onset of disease and adapt therapy
to prevent morbidity and mortality.
3. Conflict of interest
None
declared.
References
4. Johnston sl, lock
rj, gompels j. Takayasu’s arteritis: a review. J clin pathol 2002;55(7):481-486.
5. Takayasu’s arteritis.
2019.
6. Takayasu’s arteritis.
2012.
7. Keser g, aksu k, direskeneli h. Takayasu
arteritis: an update. Turk j med sci 2018;48(4):681-697.
9. Hotchi m.
Pathological studies on takayasu arteritis. Heart vessels 1992;7:11-17.
10. Tuberculosis. 2020.
11. Learn about
tuberculosis. 2020.
13. Hall s, buchbinder
r. Takayasu’s arteritis. Rheum dis clin north am 1990;16(2):411-422.
17. Rook ga, stanford jl. Slow bacterial
infections or autoimmunity? Immunol today 1992;13(5):160-164.