Unusual Case of Multiple Splenic Lesions
Abstract
Keywords: Splenic abscesses; Escherichia coli; Clinical manifestations
This case highlights an uncommon
presentation of multiple splenic abscesses in an immunocompetent patient,
emphasizing the importance of considering this diagnosis even in the absence of
classic risk factors7,8.
Case
Presentation
We
present the case of a 64-year-old Portuguese man with a medical history of type
II diabetes mellitus, managed with oral antidiabetic medication. His surgical
history included a cholecystectomy performed 15 years ago in France. He was an
active smoker (40 pack-years). He presented to the ED with a 15-day history of
supramesocolic abdominal pain, associated with anorexia, nausea and significant
weight loss. He denied any changes in bowel habits, vomiting, gastrointestinal
bleeding or urinary symptoms.
On
physical examination, the patient was febrile (temperature, 38.9°C) and had
tenderness on palpation of the left upper quadrant, with a deep palpable mass,
but no signs of peritoneal irritation. He was hemodynamically stable, with a
blood pressure of 136/76 mmHg and a heart rate of 101 beats per minute.
Initial
laboratory workup in the ED revealed normocytic/normochromic anaemia
(haemoglobin, 10.6 g/dL), leucocytosis (32.25 × 10³/µL), neutrophilia and
thrombocytosis (platelets, 853 × 10³/µL). C-reactive protein was elevated at
10.01 mg/dL. The patient underwent a sepsis screening, as illustrated in (Table
1).
Table
1:
Completed analytical study
|
Test |
Result |
Reference
range |
|
Red blood cells |
3.38 × 10⁶/µL |
4.4-6.0 × 10⁶/µL |
|
Hemoglobin |
10.6 g/dL |
13.0-18.0 g/dL |
|
MCV |
93.9 fL |
43-55 fL |
|
MCH |
31.2 pg |
27-33 pg |
|
RDW |
14.20% |
11-16% |
|
Leukocytes |
32.25 × 10³/µL |
4.0-11.0 × 10³/µL |
|
Neutrophils |
92.0% |
53.8-69.8% |
|
Eosinophils |
0.0% |
0.6-4.6% |
|
Basophils |
0.0% |
0.0-1.5% |
|
Lymphocytes |
4.0% |
25.3-47.3% |
|
Monocytes |
4.0% |
4.7-8.7% |
|
Platelets |
853 × 10³/µL |
150-400 × 10³/µL |
|
Glucose |
116 mg/dL |
82-115 mg/dL |
|
Urea |
15 mg/dL |
<50 mg/dL |
|
Creatinine |
0.40 mg/dL |
0.7-1.4 mg/dL |
|
Sodium |
135 mEq/L |
135-147 mEq/L |
|
Potassium |
3.9 mEq/L |
3.7-5.1 mEq/L |
|
ALP |
124 U/L |
40-130 U/L |
|
Gamma-GT |
111 U/L |
0-49 U/L |
|
AST |
13 U/L |
<40 U/L |
|
ALT |
4 U/L |
<41 U/L |
|
C-reactive protein |
10.01 mg/dL |
<0.5 mg/dL |
|
INR |
1.27 |
<1.2 |
|
APTT |
34.7 seconds |
24-35 seconds |
|
APTT ratio |
1.2 |
<1.2 |
|
Blood cultures |
Gram-negative bacilli: Escherichia coli (four
bottles: two aerobic and two anaerobic) |
- |
|
Antibiotic susceptibility test |
Resistant only to ampicillin
and ticarcillin |
- |
Blood
cultures were collected using four bottles: two aerobic and two anaerobic.
ALP,
alkaline phosphatase; ALT, alanine aminotransferase; APTT, activated partial
thromboplastin time (seconds); AST, aspartate aminotransferase; gamma-GT,
gamma-glutamyl transferase; INR, international normalized ratio; MCH, mean
corpuscular haemoglobin; MCHC, mean corpuscular haemoglobin concentration; MCV,
mean corpuscular volume; RDW, red cell distribution width
(Figure
1A, 1B) shows contrast-enhanced abdominopelvic CT scans revealing
heterogeneous splenomegaly with multiple hypodense, poorly enhancing
parenchymal lesions, suggestive of splenic infarctions or collections of
indeterminate nature.

Figure 1: Splenic lesions observed on CT scan
Hospitalization
in the surgery department was recommended, with empirical antibiotic therapy
(piperacillin-tazobactam and metronidazole).
Results
of the three blood cultures revealed Gram-negative bacilli (Escherichia coli),
resistant only to ampicillin and ticarcillin. Transthoracic echocardiography
excluded findings suggestive of vegetations, with a left ventricular ejection
fraction of 54% and no wall motion abnormalities, as illustrated in (Figure
2).

Figure
2:
Transthoracic echocardiogram
On the sixth day of hospitalization, a follow-up abdominal MRI showed confluence of some collections in the upper pole, measuring 6 and 8 cm in length, with no evidence of perisplenic abscess formation (Figure 3A, 3B).
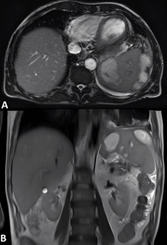
Figure
3:
Abdominal MRI
Percutaneous drainage by interventional radiology was proposed5-8 but could not be performed due to an iatrogenic pneumothorax during the procedure (Figure 4A, 4B).

Figure
4:
Complications of percutaneous drainage
Discussion
Splenic
abscesses are a rare but potentially life-threatening condition, with reported
incidence and mortality significantly reduced in the modern imaging era1-10. They are most commonly associated with
hematogenous dissemination from bacteraemia or infective endocarditis. Clinical
presentation is frequently nonspecific, which may delay diagnosis and increase
the risk of complications such as rupture and sepsis. In this case, the
presence of persistent fever, leucocytosis and left upper quadrant pain raised
suspicion for splenic pathology, later confirmed by imaging.
Contrast-enhanced
CT is the diagnostic modality of choice, although differentiation from splenic
infarction, hematoma or neoplastic lesions may be difficult. In our patient,
MRI helped clarify the diagnosis by demonstrating confluent collections
consistent with abscesses. Blood cultures grew E. coli, supporting a bacteraemia
origin, despite the absence of an identifiable primary focus or evidence of
infective endocarditis.
Management
of splenic abscesses requires both antimicrobial therapy and adequate source
control. While image-guided percutaneous drainage is a spleen-preserving option
in selected cases, it is less effective in large, multiloculated or multiple
abscesses and is associated with procedural risks. In this patient, drainage
was complicated by pneumothorax and the persistence of large collections (>7
cm) increased the risk of rupture, making splenectomy the most appropriate
therapeutic option.
This
case highlights an uncommon presentation of E. coli sepsis manifesting solely
as multiple splenic abscesses in an immunocompetent patient, emphasizing the
need for a high index of suspicion and timely definitive management.
Conclusions
This
case illustrates a rare presentation of E. coli bacteraemia manifesting as
multiple splenic abscesses in an immunocompetent patient without an
identifiable primary source. It highlights the importance of considering
splenic abscess in patients presenting with prolonged fever, leucocytosis and
left upper quadrant abdominal pain. Early imaging, prompt antimicrobial therapy
and timely escalation to definitive surgical management when conservative or
percutaneous approaches fail are essential to prevent life-threatening
complications and achieve favourable outcomes.
References
1. Chun CH, Raff MJ, Contreras L,
et al. Splenic abscess. Med (Baltimore) 1980;59:50-65.
10. Karakas S, Aydin H, Ersan Y, et al. Splenic abscess: clinical features and outcomes in 16 patients. Int J Surg 2014;12:292-296.