Unveiling the Uncommon: Cirrhosis-Induced Pleural Effusion in the Absence of Ascites
Abstract
Hepatic hydrothorax is a well-recognized complication of advanced liver disease, typically occurring in patients with ascites. However, the presentation of hepatic hydrothorax in the absence of significant ascitic fluid is very uncommon and illustrates a unique diagnostic dilemma. This case report presents a 58-year-old female with a significant history of liver cirrhosis secondary to chronic hepatitis b infection, who developed a massive right-sided pleural effusion lacking any concomitant ascites. The clinical presentation, diagnostic workup, and management of this case are discussed, highlighting the pathophysiological mechanisms underlying this unusual presentation. The case highlights the need for clinicians to maintain a high index of suspicion for hepatic hydrothorax in cirrhotic patients who exhibit respiratory symptoms, even in the absence of ascites, to ensure timely and appropriate management.
Keywords: hepatic hydrothorax; cirrhosis; pleural effusion; ascites
Introduction
Hepatic hydrothorax
is defined as the presence of a pleural effusion, typically right-sided, in
patients with portal hypertension and liver cirrhosis, occurring in the absence
of primary cardiac, pulmonary, or pleural disease. It is reported in approximately
5-11% of patients with cirrhosis, most commonly in association with ascites1. The pathophysiology of hepatic hydrothorax is
primarily attributed to the transfer of ascitic fluid through diaphragmatic
defects into the pleural cavity, facilitated by negative intrathoracic pressure
and increased abdominal pressure due to portal hypertension2. However, hepatic hydrothorax can rarely occur
without significant ascitic fluid, complicating the diagnostic
process3.
Managing hydrothorax, especially when ascites is not
present, requires an approach that includes thoracentesis for symptom relief,
diuretics for addressing fluid overload, and potentially considering liver
transplantation for patients with advanced liver disease5. This case underscores the importance of
identification and awareness of this manifestation of hepatic hydrothorax to
improve patient outcomes.
A
58-year-old female with a known history of liver cirrhosis secondary to chronic
hepatitis b infection presented to the emergency department with acute onset
dyspnea, right-sided pleuritic chest pain, and intermittent abdominal
discomfort. Her medical history is significant for esophageal varices,
hypertension, and hepatic portal vein thrombosis. She is status post inferior
vena cava (ivc) filter placement in july 2023. The patient reported a recent
travel to the dominican republic, where she experienced an episode of
hematemesis necessitating hospitalization and multiple blood transfusions due
to significant blood loss. Despite prior treatment, she has never been on
antiviral therapy for hepatitis b and has not previously consulted with a
hepatologist.
On
physical examination, the patient was found to be tachypneic (rr 34), icteric,
and mildly hypoxic. Notably, breath sounds were markedly decreased on the right
side of the thorax. The abdomen was soft, non-tender, and non-distended, with
no evidence of ascites on examination. The patient’s skin was significantly
jaundiced, with multiple excoriations noted.
Laboratory
investigations demonstrated significant hepatic dysfunction with elevated
bilirubin, increased liver enzymes, prolonged coagulopathy, and decreased
albumin. Renal function was compromised with a substantially increased serum
creatinine level. Electrolyte imbalances included hyponatremia and hypokalemia
(table 1).
Table 1: laboratory investigations on
admission
|
Parameter |
Result |
Reference range |
|
Sodium (na) |
135 mmol/l |
135-145 mmol/l |
|
Chloride (cl) |
100 mmol/l |
96-106 mmol/l |
|
Bun |
21 mg/dl |
7-20 mg/dl |
|
Potassium (k) |
3.1 mmol/l |
3.5-5.0 mmol/l |
|
Bicarbonate (hco3) |
22 mmol/l |
22-29 mmol/l |
|
Creatinine (cr) |
1.9 mg/dl |
0.6-1.2 mg/dl |
|
Alt |
125 u/l |
7-56 u/l |
|
Ast |
97 u/l |
5-40 u/l |
|
Total bilirubin |
14.8 mg/dl |
0.1-1.2 mg/dl |
|
Albumin |
1.2 g/dl |
3.5-5.0 g/dl |
|
Pt |
22 sec |
11-13.5 sec |
|
Inr |
2.3 |
0.8-1.1 |
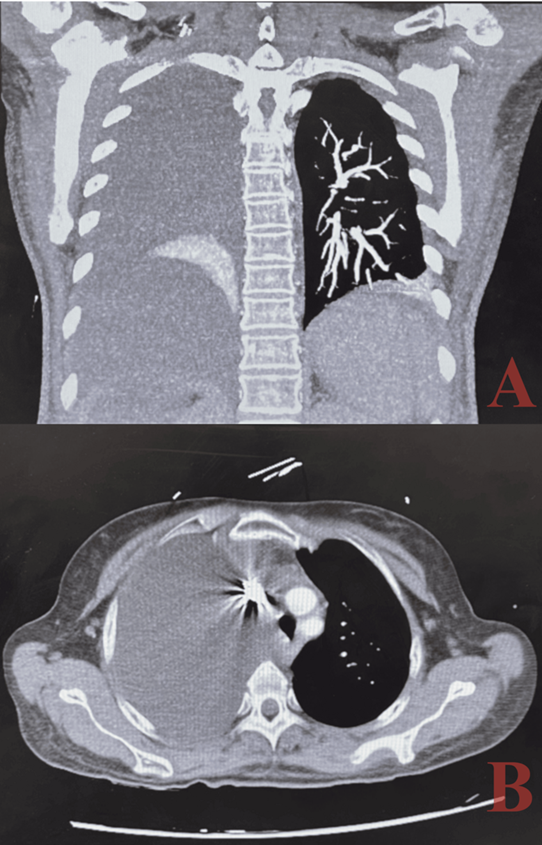
Figure 1: ct angiography imaging in coronal and axial planes demonstrating right-sided pleural effusion and lung collapse: the coronal (a) and axial (b) ct angiography images show a large right-sided pleural effusion leading to nearly complete collapse of the right lung
The differential diagnosis for the pleural effusion included transudative causes such as hepatic hydrothorax, particularly given the absence of ascites, as well as other etiologies like congestive heart failure and pulmonary embolism.
Thoracentesis was performed, yielding approximately 1.5 liters of straw-colored fluid. Analysis of the pleural fluid was consistent with a transudative effusion based on light’s criteria. Light's criteria are used to classify pleural effusions into transudates or exudates, with transudative effusions typically having a pleural fluid protein to serum protein ratio <0.5, a pleural fluid ldh to serum ldh ratio <0.6, and a pleural fluid ldh level <2/3 the upper limit of normal serum ldh6. Based on these criteria, the ratios provided indicate that the pleural fluid is consistent with a transudate (table 2).
Table 2: analysis of pleural fluid according to light's criteria
|
Parameter |
Pleural fluid |
Serum |
Ratio |
Reference range (transudate
criteria) |
|
Protein (g/dl) |
1.0 |
6.0 |
0.17 |
Pleural fluid protein/serum
protein < 0.5 |
|
Ldh (u/l) |
150 |
600 |
0.25 |
Pleural fluid ldh/serum ldh <
0.6 or pleural fluid ldh < 2/3 the
upper limit of normal serum ldh (600 u/l) |
A
post-thoracentesis chest x-ray showed re-expansion of the right lung with
stable bibasilar opacities and minimal blunting of the right costophrenic
angle. Notably, there was a small right apical pneumothorax (figure 2).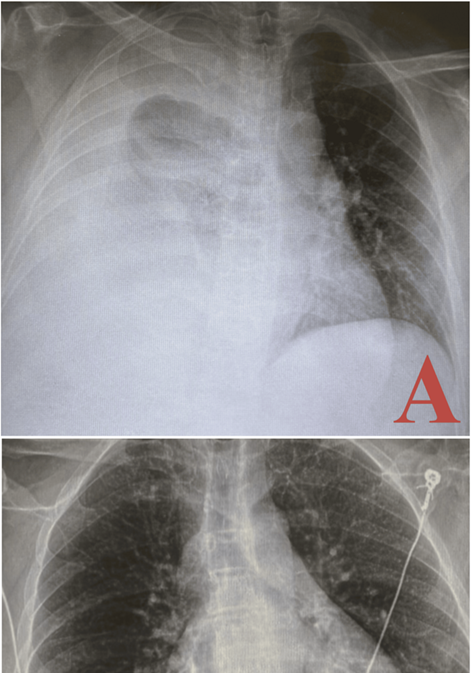
Figure 2:
chest x-rays pre- and post-thoracentesis illustrating resolution of pleural
effusion: the pre-thoracentesis chest x-ray (a) shows a large right pleural
effusion with associated near-complete collapse of the right lung and leftward
mediastinal shift. The post-thoracentesis chest x-ray (b) demonstrates the
re-expansion of the right lung, with resolution of the effusion and minimal
residual blunting of the right costophrenic angle. A small right apical
pneumothorax is also observed.
Discussion
This case of a large right-sided pleural effusion
secondary to cirrhosis in the absence of significant ascites is particularly
noteworthy due to its atypical presentation. Commonly, hepatic hydrothorax is
associated with significant ascitic fluid; however, in this instance, the
patient’s presentation with a large pleural effusion without corresponding
ascites necessitated a thorough diagnostic approach. The use of light's
criteria was instrumental in categorizing the effusion as transudative,
consistent with hepatic hydrothorax rather than other etiologies such as
exudative effusions, which might indicate malignancy or infection.
Pathophysiology
and alternative mechanisms
The pathophysiology underlying hepatic hydrothorax in
the absence of ascites remains complex and multifactorial. Several mechanisms
potentially contribute to the formation of pleural effusion without significant
ascitic fluid:
Increased
hydrostatic pressure: portal hypertension, a
relatively common complication of cirrhosis, leads to elevated pressures within
the splanchnic circulatory network. This elevated hydrostatic pressure can
extend to the pleural capillaries, promoting the transudation of fluid into the
pleural space7. Normally, this fluid
accumulates in the peritoneal cavity as ascites, but in some cases, it may
preferentially migrate into the pleural space through microscopic diaphragmatic
defects or via direct transudation due to localized pressure gradients.
Decreased oncotic
pressure: hypoalbuminemia, frequently seen in
patients with advanced liver disease, reduces plasma oncotic pressure,
facilitating fluid movement from the intravascular compartment to the
extravascular space. Albumin, a major plasma protein synthesized by the liver,
plays a crucial role in maintaining colloid osmotic pressure. In cirrhosis,
hypoalbuminemia results from impaired hepatic synthesis and increased capillary
permeability, contributing to fluid accumulation in body cavities, including
the pleural space8.
Diaphragmatic defects:
small, often microscopic, defects in the tendinous portion of the diaphragm can
act as conduits for fluid passage from the peritoneal cavity to the pleural
space. These defects may be congenital or acquired, possibly exacerbated by
increased intra-abdominal pressure due to portal hypertension. The negative
intrathoracic pressure generated during respiration further facilitates this
fluid migration. This mechanism, although typically associated with the
presence of ascites, can occur independently, leading to isolated pleural
effusions. A similar presentation of a pleural effusion in the absence of
abdominal ascites was noted in a case, in which, two patients who presented
with right-sided pleural effusions and no abdominal ascites. Both patients had
diaphragmatic defects: one was an old traumatic diaphragmatic tear and the
other a pinpoint spontaneous perforation9.
Another case describing a difficult diagnostic and therapeutic management of a
massive pleural effusion on the right side in the absence of any relevant
ascites mentions the likely direct movement of fluid from the peritoneal cavity
into the pleural space through diaphragmatic defects10.
Lymphatic
obstruction: impaired lymphatic drainage due to cirrhosis and portal
hypertension can contribute to pleural effusion formation. The thoracic duct,
responsible for draining lymph from the abdomen into the venous system, may be
compromised by elevated pressures, leading to lymphatic overflow and subsequent
transudation of fluid into the pleural cavity11.
This lymphatic dysfunction is compounded by the systemic effects of cirrhosis,
including hypoalbuminemia and altered vascular permeability.
Clinical
implications and diagnostic approach
The unusual presentation of hepatic hydrothorax
without ascites poses a diagnostic challenge. This case underscores the
importance of maintaining a high index of suspicion in cirrhotic patients
presenting with respiratory symptoms. Comprehensive diagnostic evaluation is
essential and should include:
Imaging studies:
chest radiography and computed tomography (ct) scans are pivotal in identifying
pleural effusions and assessing the extent of lung involvement. In this case,
imaging revealed a significant right-sided pleural effusion with near-total
lung collapse and mediastinal shift, underscoring the severity of the
presentation. Ct angiography additionally confirmed liver morphology consistent
with cirrhosis and excluded pulmonary embolism.
Pleural fluid
analysis: thoracentesis and subsequent analysis of
pleural fluid are critical in differentiating transudative from exudative
effusions. Light's criteria, based on pleural fluid protein and lactate
dehydrogenase (ldh) levels relative to serum values, classify the effusion as
transudative in this case. This classification is consistent with hepatic
hydrothorax and helps exclude other etiologies such as malignancy, infection,
or inflammatory conditions.
Laboratory
investigations: evaluating liver function tests,
coagulation profiles, and renal function is vital in understanding the overall
impact of cirrhosis and guiding therapeutic interventions. In this case,
significant hepatic dysfunction, including hyperbilirubinemia, hypoalbuminemia,
elevated liver enzymes, and coagulopathy, was evident. Additionally, renal
impairment and electrolyte imbalances were noted, reflecting the systemic
effects of advanced liver disease.
Management
strategies
Managing hepatic hydrothorax, especially in the
absence of ascites, requires a multifaceted approach:
Thoracentesis:
this procedure serves as a critical intervention to alleviate symptoms and improve
respiratory function12. In this
patient, successful drainage of pleural fluid and subsequent lung re-expansion
underscored the effectiveness of thoracentesis. Regular monitoring and repeat
thoracentesis may be necessary to manage recurrent effusions. Complications
such as pneumothorax, as observed in this case, highlight the need for careful
technique and post-procedural monitoring.
Diuretics:
diuretics, including spironolactone and furosemide, can help manage fluid
overload and reduce the recurrence of effusions. Their use must be balanced
against the risk of renal impairment, which is often present in cirrhotic
patients. Careful titration and monitoring of renal function and electrolytes
are essential to optimize diuretic therapy. Additionally, sodium restriction
may enhance the efficacy of diuretics in controlling fluid balance.
Transjugular
intrahepatic portosystemic shunt (tips):
for patients with refractory hepatic hydrothorax, tips can reduce portal
hypertension and decrease fluid transudation into the pleural space. This
procedure involves creating a shunt between the portal and systemic venous
circulation, thereby alleviating portal pressure. Tips has shown efficacy in
managing recurrent pleural effusions, although it carries risks such as hepatic
encephalopathy and requires careful patient selection13.
Liver transplantation:
in cases of advanced liver disease, liver transplantation remains the
definitive treatment. This option should be considered in patients with severe
hepatic dysfunction and refractory hydrothorax, as it addresses the underlying
cause and improves long-term outcomes. Pre-transplant evaluation and
optimization of the patient’s clinical status are crucial to enhance
post-transplant prognosis.
Conclusion
This
case underscores the clinical significance of recognizing atypical
presentations of pleural effusion in patients with cirrhosis. It emphasizes the
necessity for thorough diagnostic evaluations, including advanced imaging and
pleural fluid analysis using light's criteria, to understand the complex
interplay of factors contributing to pleural effusion in the absence of
ascites. The successful resolution of the effusion through thoracentesis
illustrates the effectiveness of appropriate intervention. However, it also
calls for ongoing research into the pathophysiology of such presentations and
potential preventive strategies to mitigate the risk of recurrence or
complications. An enhanced understanding of these mechanisms could lead to
improved patient outcomes and guide the development of targeted therapeutic
approaches in cirrhosis-associated pleural effusions.
References
1. chaaban t, kanj n, bou akl i. Hepatic
hydrothorax: an updated review on a challenging disease. Lung 2019;197:399-405.
2. pippard b, bhatnagar m, mcneill l, donnelly m, frew k,
aujayeb a. Hepatic hydrothorax: a narrative review. Pulm ther 2022;8:241-254.
3. kamath s, sunder a. Hepatic hydrothorax in
the absence of ascites: a diagnostic challenge. Cureus 2021;13:16650.
4. soeters
pb, wolfe rr, shenkin a. Hypoalbuminemia: pathogenesis and clinical
significance. Jpen j parenter enteral nutr 2019;43(2):181-193.
5. wilkins h, britt e, bhatnagar m, pippard b. Hepatic
hydrothorax. J thorac dis 2024;16(2):1662-1673.
6. light
rw. The light criteria: the beginning and why they are useful 40 years later.
Clin chest med 2013;34:21-26.
7. iwakiri y. Pathophysiology of portal hypertension. Clin
liver dis 2014;18:281-291.
8. kim js, kim cw, nam hs, cho jh, ryu js, lee hl. Hepatic
hydrothorax without ascites as the first sign of liver cirrhosis. Respirol case
rep 2015;4(1):16-18.
9. hartz rs, bomalaski j, locicero j, murphy rl. Pleural
ascites without abdominal fluid: surgical considerations. J thorac cardiovasc
surg 1984;87:141-143.
10. von
bierbrauer a, dilger m, weissenbach p, walle j. Hepatic hydrothorax--a rare
cause of pleural effusion that is difficult to manage. Pneumologie 2008;62(1):40-43.
11. kumar
r, anand u, priyadarshi rn. Lymphatic dysfunction in advanced cirrhosis:
contextual perspective and clinical implications. World j hepatol 2021;13(3):300-314.
12. singh a, bajwa a, shujaat a. Evidence-based review of
the management of hepatic hydrothorax. Respiration 2013;86(2):155-73.
13. copelan
a, kapoor b, sands m. Transjugular intrahepatic portosystemic shunt:
indications, contraindications, and patient work-up. Semin intervent radiol
2014;31(3):235-242.