Work Intrusion in Dermatology: A Case Report
ABSTRACT
Intrusion is a common problem in Dermatology, people
without a medical degree instruct their customers to use prescription
medications or perform procedures without the adequate knowledge of safety
parameters. Moreover, most medications can be obtained over-the-counter in
Ecuador and thus it becomes of easy access to anyone without any health-related
knowledge. Cosmeticians prescribe systemic medications for acne without knowing
dosage calculation or adverse effects; furthermore, they perform invasive procedures
or use photo-technologies without knowledge of safety parameters to avoid harm.
We will review the case of a patient who was treated
for acne by a cosmetician with isotretinoin plus tetracycline, and subsequently
underwent localized phototherapy on the face, which is not recommended
concomitantly. The complications were We will observe the complications of the
above and how the medical staff corrects the adverse effects.
Keywords:
Intrusion; Dermatology; Isotretinoin; Tetracyclines; Adverse effects
Abbreviations:
UV: ultraviolet
LED: light emission diodes
INTRODUCTION
Medical
work intrusion is common in third-world countries and occurs often in
dermatology; unqualified individuals tend to patients, performs dermatological
procedures, and prescribe medication which should be intended only for medical
use. Here we highlight a case of acne treated incorrectly by non-medical
personnel which lead to consequences which were fortunately solved by
dermatologists.
CASE PRESENTATION
A 14-year-old male patient with no significant
medical history presented with papules, pustules and nodules for about 1 year.
The patient's mother took him to a cosmetician who performed a facial and
indicated the use of 40mg of isotretinoin and 100 milligrams of minocycline
daily. Fourteen days after the treatment, the cosmiatrician performed localized
phototherapy therapy on the face. It is unknown whether this was a UVB or LED
lamp.
One day later, the patient reported pain, left
eyelid inflammation which prevented eye opening, and the appearance of erythema
as well as clear fluid-filled vesicles on the face, predominantly on the left
lower eyelid and cheek without a herpetic distribution.
Three days after start of symptoms, the patient
attended the emergency room of the Military hospital in Quito. At the time,
multiple papules forming a brownish, post-burn plaque with few mieliceric crust
were noted covering the left eyebrow, cheek, frontal, preauricular and left
malar areas (Figure 1 A&B). Futhermore, mild left hemifacial edema
was noted. 
Figure 1. A:
Plaque with a mieliceric surface on the left eyebrow and ipsilateral cheek,
papules with the same characteristics in the central frontal and left
preauricular area, accompanied by left upper and lower blepharitis. B: Anterior
view approach to lesions described above.
On laboratory the
patient presented mild leukocytosis (14,000 mm3) with neutrophilia (88%)
elevated C-reactive protein (6.4 mg/dl) and Erythrocyte sedimentation rate
(16.1 mm/h) Other laboratory values were within normal parameters
The
patient was admitted to the hospital with a diagnosis of acute II-degree
superficial burn, blepharitis, and impetiginized acne; isotretinoin and
minocycline were withdrawn. He was treated with prednisone 40 mg daily for 7
days, topical fusidic acid cream every 12 hours in facial lesions for 15 days
plus compresses with Burrow's solution once a day, and he was placed under
neurological observation due to the inadequate combination of isotretinoin plus
tetracycline. He presented a favorable evolution, with 8 days of follow-up in
hospitalization and with apparent complete recovery from the condition, he was
discharged (Figure 2).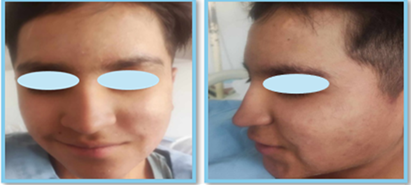
Figure 2.
A and B: Resolution of
lesions after 8 days of treatment
DISCUSSION
The
combination of tetracyclines with isotretinoin can cause intracranial
hypertension and is thus contraindicated1. Our
patient remained hospitalized under neurological observation for 8 days and
fortunately did not present any neurological signs or symptoms.
Artificial
therapeutic lamps that simulate ultraviolet radiation can produce an effect
similar to sunburn2; it is
therefore recommended that any ultraviolet radiation therapy located on the
skin should be supervised or performed by dermatologists to reduce adverse
events such as burns, pain, hyperpigmentation, among others.
Dermatologists
are trained to manage and prevent the adverse effects of isotretinoin. Among
the most important adverse effects are mucocutaneous events and teratogenicity3, thus they must be prescribed by dermatology
medical personnel for use in acne.
Topical
antibiotics and corticosteroids can be used for the management of blepharitis4, due to the environment in which we find
ourselves in Ecuador, fusidic acid cream was chosen for topical treatment for
the management of blepharitis.
CONCLUSIONS
Acne
must be treated by a dermatologist to prevent complications and to treat them
properly in case they appear. The general public should be informed that only
medical-trained personnel are qualified to prescribe systemic medications.
Drug
interactions must be studied before prescribing isotretinoin and antibiotics
such as tetracyclines since both are indicated for the treatment of acne but
must not be used concomitantly as their combination can cause neurological
damage such as pseudotumour cerebri.
Ethical permission: The
patient has given informed consent during his treatment for the publication of
this article.
Conflict of
Interest: The authors declare no conflicts of
interest.
REFERENCES
1. Berbis P. [Retinoids: drug interactions]. PubMed 1991;118(4):271-272.
2. Matsumura Y, Ananthaswamy HN. Toxic effects of
ultraviolet radiation on the skin. Toxicol Appl Pharmacol 2004;195(3):298-308.
3. Bagatin E, Costa
CS. The use of isotretinoin for acne-an update on optimal
dosing, surveillance, and adverse effects. Expert Rev Clin Pharmacol 2020;13(8):885-897.
4. Duncan K, Jeng BH. Medical management of blepharitis. Curr Opin Opthalmol
2015;26(4):289-294.